This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
(MedPage Today) -- PHOENIX -- Sooner is better for intravenous thrombolysis (IVT) given before mechanical thrombectomy for acute ischemic stroke, a meta-analysis of patient-level data from randomized controlled trials showed. While the overall.
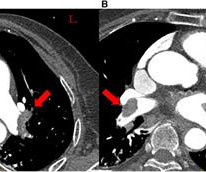
In this case report, we demonstrated that thrombus aspiration and in situ thrombolysis through the Guidezilla GEC are applicable to patients with PE in whom systemic thrombolysis is contraindicated, resulting in successful reperfusion and positive clinical outcomes.
(MedPage Today) -- PHOENIX -- Adjunctive thrombolysis with either argatroban or eptifibatide for acute ischemic stroke did not boost efficacy and contributed to risk, the MOST trial showed. When given after starting alteplase (Activase) or tenecteplase.
We aimed to create a protocol that identifies thrombolysis candidates for patients presenting with isolated dizziness.Methods:A code stroke activation protocol was implemented by the Rhode Island Hospital Stroke Committee in 08/2021. From 01/2023-06/2024 there were 0 misses. in 2021, 37.5 in 2022, 48 in 2023, and 62 in 2024.
BACKGROUND:Prior clinical trials have demonstrated the efficacy of ultrasound-facilitated catheter-directed thrombolysis (USCDT) for the treatment of acute intermediate-risk pulmonary embolism (PE) using reduced thrombolytic doses and shorter infusion durations. Circulation: Cardiovascular Interventions, Ahead of Print.
BackgroundIntravenous thrombolysis (IVT) is an effective stroke therapy that remains underused. Journal of the American Heart Association, Ahead of Print. Currently, the use of IVT in patients with recent direct oral anticoagulant (DOAC) intake is not recommended.
Thrombolysis at the spoke hospital with the patient transferred to the hub for MT is a model known as drip-and-ship. Thrombolysis dwell time was defined as the timefrom administration of thrombolysis to repeat vascular imaging. The mean time from LKN to thrombolysis was 2.2 years (range, 25.1 range, 0 to 34). hours vs 2.7
Properties of the formed thrombus may influence thrombolysis efficiency and impede recanalization success. vitro, IL-6 can was found to increase thrombin generation via monocyte tissue factor.Conclusions:Increased thrombin generation on admission is associated with unfavourable outcome at 90 days in thrombolysis treated stroke patients.
IC thrombolysis was associated with a significantly lower incidence of MACE (RR=0.65, 95% CI 0.51 Conclusion Adjunctive IC thrombolysis at the time of primary PCI in patients with STEMI improves clinical and myocardial perfusion parameters without an increased rate of bleeding. Results 12 studies with 1915 patients were included.
One of the considered and currently increasingly preferred options is intravenous thrombolysis. According to our data, intravenous thrombolysis is also an effective and safe therapy here. The effectiveness of the intervention was evaluated in two stages.
What is the association of treatment with intravenous thrombolysis (IVT) plus thrombectomy versus thrombectomy alone and outcomes modification by the time from stroke symptom onset to treatment?
The new analysis of the trial results, led by UVA Health’s Andrew Southerland , MD, found that high blood sugar shortly after thrombolysis – opening blocked arteries in the brain with a clot-busting drug – was associated with greater risk for potentially deadly brain bleeds, particularly in older patients with more severe strokes.
Background:Previous study found that compared with thrombolysis, antiplatelet did not improve outcomes but reduce the risk of symptomatic intracranial hemorrhage(sICH) for mild acute ischemic stroke(AIS) defined as National Institutes of Health Stroke Scale score 0 to 5. Stroke, Volume 56, Issue Suppl_1 , Page ATP25-ATP25, February 1, 2025.
Introduction:Emergency-department-based implementation strategies to increase thrombolysis are promising. We sought to quantify the number of hospitals with opportunities to increase thrombolysis under various tPA treatment thresholds.Methods:We used data from the 2018 State Inpatient Databases (SID) from 17 states.
Introduction:Stroke is a leading cause of disability and mortality worldwide, with thrombolysis as a critical treatment. Studies aiming to assess the outcomes of thrombolysis after ischemic stroke in LMIC were selected. Seven randomized controlled trials (RCTs) were included and analyzed independently.
NETs are proposed as a mechanism of resistance to thrombolysis. Thrombolysis was remarkably associated with higher NE positivity (average marginal effect, 6.461 [95% CI, 0.7901–12.13];P=0.02555), regardless of the origin of thrombi. BACKGROUND:Thrombosis is linked to neutrophil release of neutrophil extracellular traps (NETs).
nationwide quality initiative Target: Stroke (TS) is associated with improvement in thrombolysis frequency, timeliness, and outcome, according to a study published online Feb. 7 in JAMA Network Open.
Introduction:Intravenous thrombolysis with alteplase (tPA) or tenecteplase (TNK) is a first-line treatment for acute ischemic stroke. We reviewed stroke databases from 2017 to 2024 for patients who received IV thrombolysis with either tPA or TNK and developed sICH within 36 hours of treatment.
There were also no other complications.Conclusion:Rescue therapy in the form of prolonged low-dose thrombolysis seems to be an effective and safe alternative to therapeutic nihilism in ultra-early stroke recurrence. The incidence of intracerebral hemorrhage was 9.1% and we did not observe symptomatic intracerebral hemorrhage.
Introduction:Current guidelines suggest using intravenous thrombolysis (IVT) for patients experiencing acute ischemic stroke within 4.5 hours of symptom onset. Nevertheless, recent clinical trials have explored the possibility of extending the IVT treatment window.
hour window, and reperfusion through thrombolysis has been shown to enhance functional outcomes in patients with salvageable brain tissue beyond this timeframe.Objective:The aim of this study is to assess the efficacy and safety of thrombolysis administered more than 4.5 These modalities can identify viable brain tissue beyond the 4.5-hour
Introduction:Prior studies have demonstrated social determinants of health (SDoH) are associated with reduced rates of intravenous thrombolysis (IVT) for acute ischemic stroke (AIS), including in disadvantaged populations. 24hrs through Tufts Late Presenter Thrombolysis protocol. IVT was offered in the standard 0-4.5hr window and 4.5-24hrs
Introduction:Prior studies have demonstrated social determinants of health (SDH) are associated with reduced rates of intravenous thrombolysis (IVT) for acute ischemic stroke (AIS), including in disadvantaged populations. 24hrs through Tufts Late Presenter Thrombolysis protocol. IVT was offered in the standard 0-4.5hr window and 4.5-24hrs
Background:Patients with acute ischemic stroke and a large vessel occlusion (LVO) admitted to primary stroke centers (PSC) often require inter-facility transfer for thrombectomy.
Introduction:The tenecteplase versus standard of care for minor ischemic stroke with proven occlusion (TEMPO-2) trial showed that patients presenting with minor deficits up to 12 h do not benefit from intravenous thrombolysis. h, if they were not eligible for standard-of-care thrombolysis. mg/kg) or non-thrombolytic standard of care.
2) Creation of a multidisciplinary Thrombolysis Focus Group to analyze data and improve processes. Additional monthly quality improvement meetings were held to discuss all thrombolysis cases with times over our median. 3) Reduction of EMR barriers to recognize metric exclusion criteria and document accordingly. in 2020, to 31.9%
The goal of the trial was to compare the efficacy and safety of large-bore mechanical thrombectomy (LBMT) with catheter-directed thrombolysis (CDT) in the treatment of intermediate-high risk pulmonary embolism (PE).
Aside from the use of thrombolysis for stroke on awakening. Intravenous tenecteplase has been shown to be noninferior to alteplase, with a meta-analysis suggesting superiority,1 and although tenecteplase has been used off label, it is replacing alteplase as the preferred thrombolytic agent for the treatment of acute stroke.
The effectiveness and safety of intravenous thrombolysis (IVT) for acute ischemic stroke in these cases, particularly those involving large vessel occlusions, are debated. Stroke, Volume 56, Issue Suppl_1 , Page AWP9-AWP9, February 1, 2025. Background:Acute ischemic stroke can result from extracranial arterial dissection.
Introduction:Trials using advanced imaging have shown a benefit from intravenous thrombolysis in patients with wake-up stroke, but real-world data is limited. 71% of stroke activations had a final diagnosis of ischemic stroke; 32% of cases were eligible per protocol and treated with thrombolysis. Median admission NIHSS was 6.
Introduction:IV thrombolysis is a proven treatment for acute ischemic stroke (AIS), but it is still underutilized in real-world clinical practice. Trends in IV thrombolysis rate were respectively analyzed for all patients (cohort 1), patients who arrived at the hospital within 4.5
mg/kg]) comparing IVT with placebo or standard treatment from the EOS (Evaluation of Unknown-Onset Stroke Thrombolysis trial) data set. mg/kg]) comparing IVT with placebo or standard treatment from the EOS (Evaluation of Unknown-Onset Stroke Thrombolysis trial) data set.
Most respondents (88%) agreed there were barriers to acute stroke thrombolysis in the region. Among 51% of countries surveyed, no acute thrombolytic treatment was provided for acute stroke in the 2021 calendar year. Only 1 center treated >100 cases per year.
To compare the treatment outcomes among percutaneous mechanical thrombectomy (PMT) with AngioJet, Catheter-directed thrombolysis (CDT), and a combination of both.
Whether intravenous thrombolysis (IVT) is safe and effective for acute ischemic stroke (AIS) patients with CAA is largely unknown.Methods:This was an explorative analysis of a nationwide database of hospitalizations in the United States.
Background and Aims:Endovascular treatment (EVT) alone has been confirmed to be non-inferior to intravenous thrombolysis (IVT) followed with EVT in acute ischemic stroke (AIS) due to large-vessel occlusion of the anterior circulation. Stroke, Volume 56, Issue Suppl_1 , Page AWP253-AWP253, February 1, 2025.
Background and Purpose:Whether imaging markers of cerebral small vessel disease on computed tomography (CT-CSVD) relates to early clinical outcomes after intravenous thrombolysis for acute ischemic stroke remains not well understood. Stroke, Volume 56, Issue Suppl_1 , Page AWP6-AWP6, February 1, 2025. 1.02; score 2: OR 0.46, 95%CI 0.26-0.83;
SETRAC has demonstrated its efficacy in improving thrombolysis rates in patients with acute ischemic stroke. We performed linear analyses to evaluate the increase in the percentage of patients receiving thrombolysis, and those treated within 45 minutes.Results:31 hospitals reported treating a total of 93,688 patients from 2014-2023.
Objectives:To examine whether thrombolysis care metrics have improved in all races and ethnicities with the launch and advance of Target: Stroke (TS) national quality initiatives.Methods:This cohort study included patients presenting to Get With The Guidelines (GWTG)-Stroke participating hospitals within 4.5
Introduction:The benefit of intravenous thrombolysis for acute ischemic stroke declines with longer time from symptom onset. Intravenous thrombolysis showed clinical benefit if it was administered within 2h 20min after symptom onset. Stroke, Volume 55, Issue Suppl_1 , Page A22-A22, February 1, 2024.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content