This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
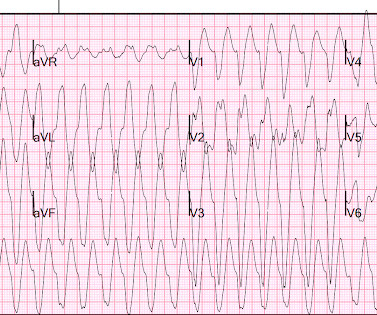
Ambulatory electrocardiography (ECG) monitoring revealed recurrent polymorphic ventricular tachycardia (PMVT). The patient presented with recurrent palpitations and pre-syncope, with no chest pain.
Here is her ECG: Regular Wide Complex Tachycardia. Could it be atrial tachycardia with RBBB and LPFB aberrancy? Here it is: There is sinus with normal conduction, very different from her tachycardia. Severely decreased LV function. What do you think? What do you want to do? She was not on any medication that could cause this.
Then I always look to see if the initial deflection of the QRS has a lot of voltage change per change in time (seen in tachycardias that are initiated from above the ventricle because the propagate through fast conducting purkinje fiber. Tachycardia exaggerates ST Elevation in LBBB and Paced rhythm 5. Pacemaker mediated tachycardia!
Here is the 12-lead ECG: Wide complex tachycardia What do you think? His pulse on the monitor suddenly went down to 140 and another 12-lead ECG was recorded: Sinus tachycardia at a rate of 143 There are peaked T-waves typical of hyperkalemia The K returned at 6.9 Blood pressure was 117/80, pulse 161, Resp 45, SpO2 100 on oxygen.
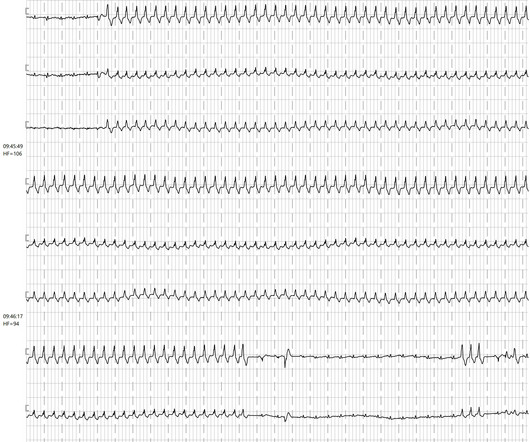
We see here a wide complex tachycardia with a frequency of approx. The short VT after the end of the sustained ventricular tachycardia with the same QRS morphology also indicates a ventricular origin of this arrhythmia. 105-110 beats per minute that lasts for a good minute.
ECG#1 There is a regular tachycardia with a ventricular rate of about 180 bpm. Smith comment : When there is a regular wide complex tachycardia, first assess whether it is sinus or not. Put shortly is SVT with "Shark Fin STE" and not ventricular tachycardia. An ECG was recorded immediately and is shown below. Is there OMI?
(MedPage Today) -- CHICAGO -- For patients with ventricular tachycardia (VT) and ischemic cardiomyopathy, going right to catheter ablation improved outcomes compared with trying antiarrhythmic drugs first, the VANISH2 trial showed. Death or.
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Description : Regular Wide Complex Tachycardia at a rate of about 160. SVT with aberrancy?
Cingolani, director of Cardiogenetics and Preclinical Research in the Department of Cardiology in the Smidt Heart Institute at Cedars-Sinai, is exploring new ways to help patients with ventricular tachycardia (VT), a recurring, abnormally fast and irregular heartbeat that starts in the lower chambers, or ventricles, of the heart.
The ECG : The first impression is that is a regular WIDE COMPLEX TACHYCARDIA. It pays to take a moment to consider the possibility of REGULAR REALLY WIDE COMPLEX TACHYCARDIA (RRWCT) before making a treatment decision. So, we can assume the patient was probably being treated for angina, heart failure, and hypertension.
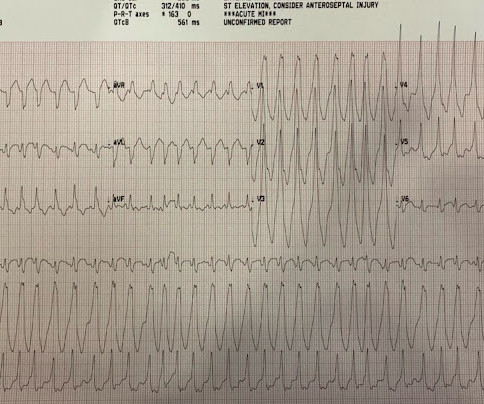
A prehospital 12-lead was recorded: There is a regular wide complex tachycardia. The computer diagnosed this as Ventricular Tachycardia. There is a wide complex regular tachycardia at a rate of 226. Toothache, incidental Wide Complex Tachycardia Could it be fascicular VT or Bundle Branch VT ( i.e., idiopathic VT )?
There is a regular narrow complex tachycardia. Thus, it is supraventricular tachycardia. It is important to remember that SVT includes Sinus Tachycardia! Sometimes even Wide Complex Tachycardia is Sinus. See this case in which Lewis leads were necessary to figure this out: Wide Complex Tachycardia.
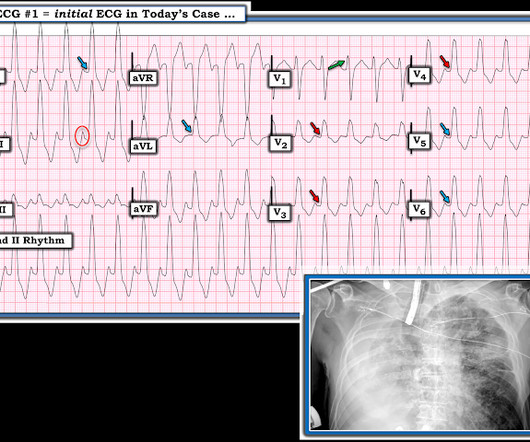
== — CLICK HERE — for a V ideo presentation of this case! Below are slides used in my video presentation. For full discussion of this case — See ECG Blog #220 — == The long lead II rhythm strip shown in Figure-1 was obtained from an 51-year-old man who presented to the ED ( Emergency Department ) with "palpitations" that began 1 hour earlier.
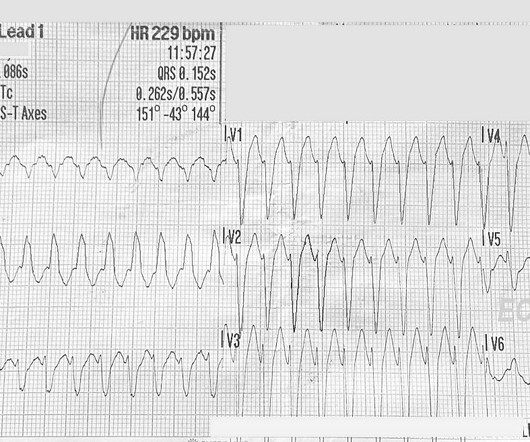
ECG Number 1, 11:57 a.m.: There is a wide-complex tachycardia at a rate of about 230 bpm. We do not have information about her past medical history. We will update this post if we receive information about her outcome. The QRS is.15 15 seconds (150 ms). The QRS frontal plane axis is leftward.
Distribution Variance of Focal Atrial Tachycardia Foci and Long-Term Outcomes After Ablation. ABSTRACT Introduction The distribution of the origin of focal atrial tachycardia (FAT) in patients with different ages have not been clearly elucidated.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
A multicenter study has described and validated a new strategy for guiding ablation procedures in patients with complex tachycardias. This type of procedure is frequently used to treat ventricular tachycardias originating in areas affected by scarring after a myocardial infarction.
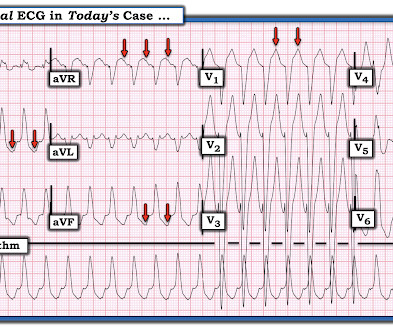
I find AV dissociation in VT to be very difficult to differentiate from artifact, as there are always random blips on tachycardia tracings. Read this post: Idiopathic Ventricular Tachycardias for the EM Physician 2. The 15th beat (2nd beat of V1-V3) appears to be a fusion beat , which is all but diagnostic of VT.
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation. What to do?
Patients with post-COVID-19 vaccination postural orthostatic tachycardia syndrome (POTS) all have preexisting conditions, according to a study published in the January issue of Heart Rhythm.
Among patients with ventricular tachycardia and ischemic cardiomyopathy, catheter ablation as an initial therapy led to a lower risk of adverse outcomes than antiarrhythmic drug therapy.
Differentiating between atypical atrioventricular node re-entrant tachycardia (aAVNRT) and orthodromic reciprocating tachycardia (ORT) utilizing a septal accessory pathway is a complex challenge.
The ECGs show a wide complex, irregularly irregular tachycardia. At that time, he presented via EMS and had received magnesium and lidocaine prehospital for concerns of ventricular tachycardia. On arrival to the ED, he was noted to be in a wide complex tachycardia with a rate in the 240s.
Scar-related re-entrant atrial tachycardias and atrial fibrillation (AF) are the most common types of AA, but focal atrial tachycardias, atrioventricular re-entrant tachycardia using an accessory pathway and atrioventricular nodal re-entrant tachycardia are also encountered.
Tachycardia of >140 (AOR=7.50, 95% CI: 1.36, 41.57), any degree of left ventricular dysfunction, Killip class IV (AOR=6.03, 95% CI: 1.27, 28.61), and non-initiation of betablockers (AOR=0.17,95% CI: 0.05, 0.63) were significantly associated with increased in-hospital mortality. Percutaneous Coronary Intervention was performed for 12.3%
BACKGROUND:Current outcomes from catheter ablation for scar-dependent ventricular tachycardia (VT) are limited by high recurrence rates and long procedure durations. Circulation, Ahead of Print.
The goal of the VANISH2 trial was to compare endocardial catheter ablation with conventional antiarrhythmic drug (AAD) therapy as a first-line treatment for infarct-related ventricular tachycardia (VT) in ischemic cardiomyopathy.
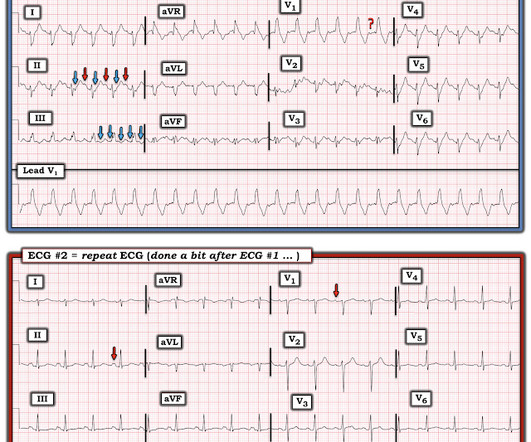
QUESTIONS: Is this rhythm too fast to be sinus tachycardia? However, until such time that we know for certain — I think it best to simply describe what we see: PEARL # 1: Realize that for any tachycardia — there are 6 Parameters that need to be assessed. Are flutter waves hidden within the QRS and T waves? s in Figure-2 ).
Clinical introduction A woman in her 60s with non-obstructive coronary artery disease, aortic valve replacement and aortic arch repair, chronic diastolic heart failure and paroxysmal atrial fibrillation (AF) and flutter (AFL), presented with 3 days of sustained palpitations that felt similar to prior episodes of AF/AFL.
Abstract Introduction Understanding the spatiotemporal location of the spontaneous termination of ventricular tachycardia (VT) may provide new insights for ablation.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. During the next 24 hours, she experienced periods of complete AV block with a ventricular escape rhythm in the 20s. She was started on isoprenalin (isoproterenol). The following ECG was recorded during one of these episodes of VT.
But it is not disorganized enough to be polymorphic ventricular tachycardia. Learning Points: Wide complex irregularly irregular tachycardias include PMVT, AF with WPW, and AF with aberrancy. See our other cases of AF with WPW: A young man with another episode of tachycardia. What do you want to do? Smith : I always cardiovert.
She was awake, alert, well perfused, with normal mental status and overall unremarkable physical exam except for a regular tachycardia, possible rales at both bases, some mild RUQ abdominal tenderness. Thus, I believe it is a regular, monomorphic, wide complex tachycardia. Or it could simply still be classic VT. What is the Diagnosis?
These result in diagnoses such as postural orthostatic tachycardia syndrome and orthostatic hypotension. Because CBF is not easy to measure, rises in heart rate or drops in blood pressure are used as proxies for abnormal CBF.
If a wide complex tachycardia occurs, the probability is very high that it is a ventricular tachycardia (approx. Here we see a broad complex tachycardia that looks like an RBBB + LAFB, which is regular. 80%, in patients with a previous myocardial infarction (.) In this constellation, 3 causes must be considered: 1.
C ASE C onclusion : I lack detailed follow-up from today's case — other than knowing that the Atrial Tachycardia was controlled. This type of Wenckebach response that may be seen with atrial tachycardia ( or atrial flutter ) — is often physiologic, as a result of the rapid atrial rate that occurs with these arrhythmias.
I was sent the ECG in Figure-1 initially told only that it was obtained from an older man with palpitations. The cardiology team thought the rhythm was an SVT ( S upra V entricular T achycardia ) with QRS widening as a result of aberrant conduction.
Heart rates are easier to monitor today than ever before. Thanks to smartwatches that can sense a pulse, all it takes is a quick flip of the wrist to check your heart. But monitoring the cells responsible for heart rate is much more challenging—and it's encouraged researchers to invent new ways to analyze them.
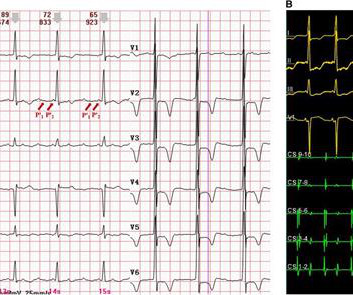
However, widely split P' waves in focal atrial tachycardia (AT) on a surface electrocardiogram (ECG) have rarely been reported. An electrophysiological study showed that the tachycardia arose from the left atrial appendage (LAA) and was conducted through two distinct pathways.
On the monitor patient had wide-complex tachycardia. Differential is ventricular tachycardia versus supraventricular tachycardia with aberrancy versus sinus tachycardia with a aberrancy. After the patient was stabilized with supportive care, the heart rate gradually slowed, confirming sinus tachycardia.
Even with tachycardia and a paced QRS duration of ~0.16 (J Am Coll Cardiol. second I immediately knew there is no way this relative increase in QT duration ( compared to the R-R interval ) is going to be "normal". 2 Quick Approximations that I Use: As I discuss in My Comment in the March 19, 2019 post in Dr.
The ECG in Figure-1 — was obtained from a middle-aged woman with positional tachycardia and diaphoresis with change of position from suprine to sitting. My THOUGHTS on the ECG in Figure-1: The rhythm is sinus tachycardia at ~105/minute ( ie, The R-R interval is regular — and just under 3 large boxes in duration ).
when the usual negative P wave deflection of sinus tachycardia is nowhere to be found in lead V1 )? While of course possible for the rhythm in ECG #1 to be either AFlutter or fascicular VT — sinus tachycardia immediately becomes a much more likely possibility once we know that this patient is critically ill with multisystem disease.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content