This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
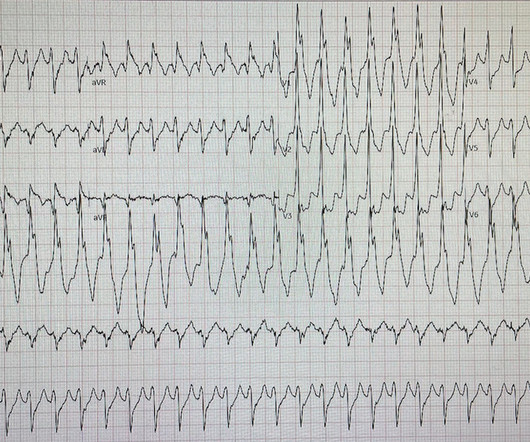
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Cardiac output (CO) was being maintained by the tachycardia.
Ultimately the patient went to Cath and was found to have multi-vessel obstructive coronary disease with an acute LCX culprit vessel, which was stented. Readers of the Smith ECG Blog will probably recognize this a very subtle inferior OMI. Corresponding echocardiogram demonstrated LV systolic dysfunction with an EF 30%.
It is of an elderly woman who complained of shortness of breath and had a recent stent placed. Also, we know the patient had a stent. This was what was found: She had been at a different hospital less than a week ago at which time she had an an RCA stent for an lesion that had TIMI-3 flow. What do you think?
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Here is his ED ECG: There is sinus tachycardia. He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
They had a history of non-ischemic cardiomyopathy (EF 30%), as well as PCI with one stent. Initial ECG in the ED: Presenting ECG : Wide-complex tachycardia at a rate about 200. This is overwhelmingly likely to be ventricular tachycardia, even if only age and medical history are considered.
This can initiate ventricular arrhythmias like polymorphic ventricular tachycardia (PMVT). Background:R-on-T phenomenon occurs when an electrical stimulus is delivered at a critical point during ventricular repolarization.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. Does this change your interpretation?
This led to immediate cath lab activation — which revealed total occlusion of a large 1st diagonal branch that was stented. == Below is the ECG of Patient #3 — recorded from a 35-year old man with sudden, new-onset CP. NOTE #1: Sinus tachycardia is not usually seen in an uncomplicated acute MI.
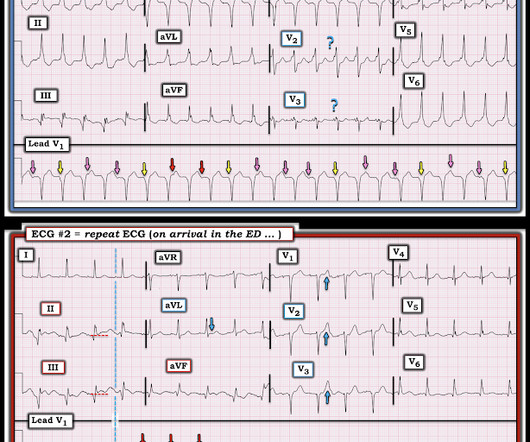
This is ischemic ST depression, and could be due to increasing tachycardia, with a heart rate over 130, but that is unlikely given that the patient is now complaining of crushing chest pain and that there was tachycardia all along. There is widespread ST depression. Figure-1: Comparison of the first 2 ECGs in today's case.
Notice there is tachycardia. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia. In this case, the patient had failed to take his atenolol in the AM and was having reflex tachycardia in addition to ACS. The OM-1 was opened and stented, then the LAD was stented 3 days later.
An EKG was repeated around midnight: By itself, this ECG is not diagnostic of anything besides sinus tachycardia, and could be called normal (although there is ST segment straightening in the anterior leads, which should always prompt suspicion). The conventional computer algorithm called “ sinus tachycardia, otherwise normal EKG ”.
There is sinus tachycardia. It was stented. I saw this as I was reading a large a stack of ECGs: What do you think? The T-waves are slightly peaked, suggesting hyperkalemia. But what is atypical is that the T-wave in V3 towers over the R-wave. The QTc is 462 ms. The possibility of anterior STEMI was not noticed during patient care.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia. It was stented. He wrote most of it and I (Smith) edited.
Prior ECG available on file from 2 months before: We do not know the clinical events happening during this ECG, but there is borderline tachycardia, PVCs, and likely some evidence of subendocardial ischemia with small STDs maximal in V5-6/II, slight reciprocal STE in aVR. Culprit lesion was reduced to 0% and stented.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. No appreciable skin pallor. He reported to be a social drinker, but used tobacco products daily. Here is the time-zero 12 Lead ECG.
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. It was opened and stented with a door to balloon time of about 120 minutes (this is long for STEMI, but very short for a high risk Non STEMI). If it is MI, is it type 1 or type 2?
Cath done around 4pm next afternoon: Acute culprit lesion: LCX 99%, TIMI 1 flow, stented Also LAD 50%, TIMI 3 flow, which was also stented And chronic RCA occlusion with collaterals (no information is in the cath report regarding where the collateral flow is from, for example if collateral flow was from the LAD or LCX).
Past medical history includes coronary stenting 17 years prior. I find AV dissociation in VT to be very difficult to differentiate from artifact, as there are always random blips on tachycardia tracings. Read this post: Idiopathic Ventricular Tachycardias for the EM Physician 2. Initial ED ECG: What do you think?
Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. C linically — the rhythm we see in the long lead II of ECG #3 behaves similar to MAT, even though there is no tachycardia. In the available view, the RCA appears fully occluded. To our knowledge, the patient did well.
INTERVENTION * Successful angioplasty and stenting (drug eluting) of the mid LAD * Successful angioplasty of the ostial 1st diagonal Learning points: 1. That said, against acute PE — is the inconstancy of this patient's symptoms — the lack of tachycardia — and the lack of any other ECG signs of acute RV strain.
Patients with repaired tetralogy of Fallot (rTOF) are at risk of sudden cardiac death (SCD) primarily due to ventricular tachycardias (VT). Prophylactic VT ablation is performed in this setting as stented valves may shield SCAIs from catheter ablation.
2) Tachycardia to this degree can cause ST segment changes in several ways. First , there can simply be diffuse ST depressions (which obligates reciprocal STE in aVR) associated with tachycardia which are not indicative of ischemia. Serial troponin T measurements rose from zero to 2.80 ng/mL over the next 10 hours.
The patient was referred immediately for cath which revealed RCA occlusion that was stented. I completely agree with Dr. Nossen that in this patient with new CP and sinus tachycardia with LAHB — that the T waves in each of the inferior leads are hyperacute ( ie, clearly disproportionately "bulky" given size of the QRS in these leads ).
After the episode of VT and the troponin results the patient was taken to the cath lab: complete occlusion of the RCA with TIMI 0 flow, which was stented. So now there was ACS + electrical instability, another indication for emergent angiogram. He also had 70% lesion of his LAD. Peak troponin was 16,500 ng/L.
This was stented. See here for management of Polymorphic Ventricular Tachycardia , which includes Torsades. In multivariate analysis, serum potassium level was negatively and age positively related to ventricular tachycardia. After pacing, there was no recurrence of Torsades. The patient stabilized. mEq/L: The STE is resolved.
pre-existing, stable atherosclerosis) amidst any state of global duress – to include hypertension, hypoxia, tachycardia, hypotension, sepsis, and GI bleed, for example. Advanced multi-vessel disease was found with stents deployed to the mid-LCx (80% stenosis), D1 (90% stensosis), and the pLAD (95% stenosis).
Although the shock is no doubt partly a result of poor pump function, with low stroke volume, especially of the RV, it should be compensated for by tachycardia. He was successfully stented. Cardiac output is stroke volume x rate, so this patient needs a higher heart rate. This is a perfect indication for atropine.
Here is another proven left main occlusion in a young woman who presented with sudden pulmonary edema, had this ECG recorded, then arrested and was resuscitated after 30 minutes of CPR: This has sinus tachycardia with RBBB and LAFB, and STE in V2-V6 as well as I, aVL This pattern could just as easily be seen in LAD occlusion.
Submitted anonymously, written by Willy Frick A man in his 70s with a history of remote MI (details unavailable) and prior stent placement presented to cardiology clinic for routine follow up. This proves AV dissociation, and by extension ventricular tachycardia. The current ECG shows sinus tachycardia with old inferior infarct.
The abnormal heart rhythms can further lead to death because of ventricular tachycardia and ventricular fibrillation. A completely blocked artery is located, a wire is inserted through it, the clot is sucked, the narrowing is widened with a balloon, and then a stent (stainless steel wire mesh) is placed to maintain consistent flow.
August 2024 Approvals Minima Stent System (P240003) (Approval Date: August 28, 2024) The Minima Stent System is an expandable cobalt-chromium metal mesh tube to reopen blood vessels in neonates, infants, and children with Coarctation of the Aorta and Pulmonary Artery Stenosis, specifically designed to expand as younger patients grow.
The CAG showed a 99% thrombotic lesion of the proximal RCA, which was stented. The patient in today's case was lucky to re-perfuse. He remained chest pain free and underwent coronary angiography the following day. Due to rapid spontaneous reperfusion, high sensitivity troponin I peaked at just under 5000 ng/L.
The thrombus was aspirated and the distal RCA was stented. The patient waited another three hours in the ED until the cath lab was ready to accept him. 6 hours after his initial presentation, he went to the cath lab: There is a filling defect consistent with thrombus in the distal RCA. There was TIMI 2 flow distal to the thrombotic occlusion.
He had undergone stenting of the LAD several weeks ago (unclear whether elective for stable symptoms, or in response to acute coronary syndrome). It is a wide complex regular tachycardia at a rate of 120. Is it ventricular tachycardia? It is a wide complex regular tachycardia at a rate of 120. He appeared critically ill.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content