This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
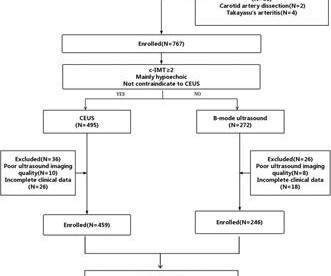
Materials and methods This retrospective study evaluated 705 patients with low and intermediate carotid stenosis who underwent B-mode and CEUS from November 2021 to April 2023. Results This study included a total of 705 patients with low and intermediate carotid stenosis, of which 394 were symptomatic patients (with a mean age of 71.03 ± 10.48
Objectives To investigate the reliability and agreement of hand-held ultrasound devices (HUDs) compared with conventional duplex ultrasound (HIGH) in examination for carotid stenosis in patients with suspected transitory ischaemic attack (TIA) or ischaemic stroke.
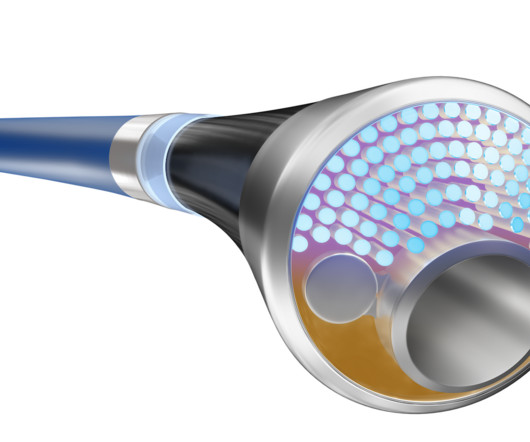
Coronary Intravascular Ultrasound (IVUS) equipment consists of an IVUS catheter, pullback device and the imaging console. In the geometry, the size of the plaque, its relationship to luminal stenosis, arterial remodeling and eccentricity can be evaluated. Incomplete stent apposition can be detected by intravascular ultrasound.
Bedside cardiac ultrasound with no obvious wall motion abnormalities. Because the pathologist determines the degree of stenosis by dividing the lumen area by the total area, the degree of stenosis will be overestimated. The angiographer uses a denominator that is too small, thereby underestimating the degree of stenosis.
We report a case of TRAD in the early postoperative period, which was successfully managed with intravascular ultrasound-assisted endovascular intervention.Case presentationA 38-year-old man underwent HLA-compatible living kidney transplantation. Most cases are managed by operative repair.
Food and Drug Administration (FDA) has granted 510(k) clearance for its first-of-a-kind, AI-powered AISAP CARDIO point-of-care ultrasound (POCUS) software platform. We know that structural heart disease and heart failure are the leading causes of hospitalization and morbidity in the U.S.
Background:Carotid stenosis has been associated with stroke and cognitive impairment. It remains unclear if hypometablism, a marker for neurodegeneration, may be in the mechanistic pathway in the association between carotid stenosis and cognitive decline. Stroke, Volume 56, Issue Suppl_1 , Page ATP215-ATP215, February 1, 2025.
The innovative feature of the Philips catheter is that both the atherectomy and lithotripsy are laser-driven. Patients will be followed for 12 months. This innovative approach to vessel preparation could improve patient outcomes while minimizing the need for multiple therapies and interventions.
510(k) clearance secured from FDA allows for EIQ’s AI-enabled solution, EchoSolv AS, to be marketed and sold in the USA Clearance marks a major milestone and will allow for rapid commercial scale-up EIQ is in advanced discussions with a range of US healthcare providers around the potential uptake of EchoSolv AS Working alongside US consultancy to obtain (..)
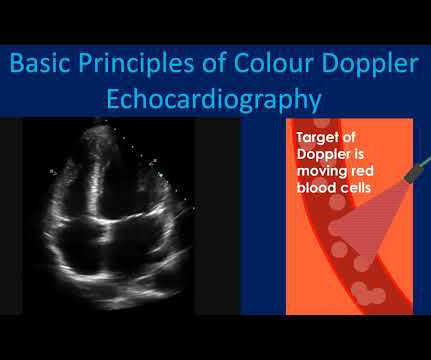
The principle of Doppler is that the frequency of sound wave coming from an object which is moving towards the ultrasound probe increases while that from an object moving away from the probe decreases. Colour Doppler echocardiography receives the ultrasound signals reflected from moving red blood cells in the heart.
However, the patient's cardiac Doppler ultrasound indicated poor cardiac contractions, and extracorporeal membrane oxygenation (ECMO) was started immediately. Fortunately, there was no obvious stenosis in the right coronary artery.
Six-month angiographic follow-up with optical coherence tomography and intravascular ultrasound was available in 74 patients. Intravascular ultrasound findings showed no difference in mean vessel area at the lesion site from baseline to follow-up in the scoring balloon group (16.82.9 versus 6.31.5 mm2;P=0.65), mean scaffold area (7.81.5
Fetal aortic valvuloplasty is considered for fetuses with severe valvar aortic stenosis and echocardiographic features suggesting a risk of progression to hypoplastic left heart syndrome. Currently all procedures are done percutaneously under ultrasound guidance following maternal spinal or epidural anaesthesia. Esch, Lynn A.
confirmed by magnetic resonance angiography (MRA), computer tomography angiography (CTA) or carotid ultrasound within the past year and had their blood acoustic vibration signatures recorded for one minute. These patients had varying CA conditions (atherosclerosis, dissection, normal, etc.)
Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. However, one can certainly imagine that many thromboses of non-obstructive lesions completely lyse and do not leave a stenosis on same day or next day angiogram.
Bedside ultrasound with no apparent wall motion abnormalities, no pericardial effusion, no right heart strain. Two ECG patterns were described by the original investigators in 1982 as being consistent with a Wellens’ Syndrome prediction of high-grade LAD stenosis. Course : Aspirin 325mg, chemistry, CBC, troponin panel all ordered.
Or is it a very tight stenosis that does not allow enough flow to perfuse myocardium that has a high oxygen demand from severely elevated BP? And angiographers tell me that it is sometimes difficult to say for certain based on angiogram alone, without intravascular ultrasound or, better yet, optical coherence tomography.
1.196 x STE60 in V3 in mm) + (0.059 x computerized QTc) - (0.326 x RA in V4 in mm) Third, one can do an immediate cardiac ultrasound. A bedside ultrasound was done by an emergency physician and simultaneously read by a cardiologist. The patient had a critical LAD stenosis. greater than 23.4 is likely anterior STEMI).
Smith comment: This patient did not have a bedside ultrasound. Had one been done, it would have shown a feature that is apparent on this ultrasound (however, this patient's LV function would not be as good as in this clip): This is recorded with the LV on the right. What should be done? Should the cath lab be activated?
ICASLVO is characterized by the presence of residual focal fixed stenosis or reocclusion following endovascular treatment or evidence of distal hypoperfusion or watershed infarction on followup imaging. ICASLVO is a significant contributor to acute ischemic stroke, with varying prevalence rates across regions.
Although indexing effective orifice area (EOA) by body surface area (BSA) is recommended, this method has several disadvantages, since it corrects by acquired fatty tissue. Our aim was to analyze the value of.
The updated workflow indicates that direct imaging guidance, such as ultrasound, may be used as an alternative to fluoroscopy. "As 1 These included one pseudoaneurysm, one PV stenosis and one hematoma.1 This is the most commonly used ablation catheter in the world for RF ablation and is fully integrated with the CARTO 3 System.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Takotsubo is a sudden event, not one with crescendo angina. Learning Points: 1.
Methods of vessel imaging were carotid duplex ultrasound, CTA, and MRA. Overall, nonstenotic carotid stenosis ipsilateral to ischemic stroke was found in 33.5% (255/761) CS patients vs 19.2% (152/790) KS patients. In formal meta-analysis, the summary risk ratio for nonstenotic carotid plaque in CS vs KS patients was 1.54 (95%CI 1.15-2.05)
Under ultrasound guidance, her PT disappeared when the posterior auricular vein collapsed under applied pressure and returned when the pressure was released. Catheter venography showed an enlarged right posterior condylar vein (PCV) and right IJ stenosis. A CT venogram revealed left IJ stenosis. mm in its widest dimension).
The left circumflex had 80% proximal stenosis with minimal luminal irregularities in the mid to distal portion. An intravascular ultrasound was also performed, which was negative for vessel dissection. After guidewire crossing, balloon angioplasty was performed, and a drug-eluting stent was deployed.
The primary efficacy outcome was the composite of no occlusion in the treated segment assessed at serial duplex ultrasound examinations or no reintervention needed to maintain patency within 6 months. Secondary outcomes, including Villalta score, quality of life, and safety outcomes, were also assessed.
My opinion was that it was not a cath lab case, but I did suggest they do a bedside ultrasound to look for an anterior wall motion abnormality. I had not seen the cardiac ultrasounds at this time. I did not have more information at the time. To the ED providers, the patient denied CP, SOB, or drug use.
Angiogram Left main: Severe calcific stenosis of ostial and distal left main. LAD: large caliber vessel with severe calcific stenosis of the proximal LAD with TIMI2 flow. There are large caliber diagonal branches with no significant stenosis. Mid LAD has another area of focal moderate stenosis.
There was an old ECG for comparison: One year prior with no ST segment abnormalities A bedside cardiac ultrasound was done by the emergency physician. LM: No significant stenosis. LAD: luminal irregularities with a 40% stenosis at the take-off of a D3. LAD: luminal irregularities with a 40% stenosis at the take-off of a D3.
During medical school, one of the classic bedside exam questions we get is how to differentiate the valve issues of aortic stenosis and mitral regurgitation, which produce similar but different murmurs when you listen with a stethoscope. “How can you tell the difference between aortic stenosis and mitral regurgitation at the bedside?”
The LAD has diffuse disease with a few areas of moderate stenosis but no flow-limiting lesions. On intravascular ultrasound (IVUS), the mid RCA plaque was described as "cratered, inflamed, and bulky," and the OM plaque was described as "bulky with evidence of inflammation and probably ulceration."
History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.” Left main? 3-vessel disease?
The cardiologist called this 20% stenosis. Fortunately, this operator used intravascular ultrasound (IVUS). Eagle eyed readers might notice a slightly scooped out appearance of the proximal LAD in the above view, right at the head of the top left green arrow. An angiogram is a " lumenogram " and does not "see" the extraluminal plaque.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. This is written by Willy Frick, an amazing cardiology fellow in St. He described it as "10/10" intensity, radiating across his chest from right to left.
The ways to tell for certain include intravascular ultrasound (to look for extra-luminal plaque with rupture) or "optical coherence tomography," something I am entirely unfamiliar with. distal stenosis or occluded small branches), and 3) nonischemic causes for myocyte injury (e.g., pulmonary embolism, sepsis, etc.), myocarditis).
Femoral artery and external jugular vein access were obtained using the Seldinger technique under ultrasound guidance and did not require a surgical cut down. MRI Brain and MR Brain venogram imaging was performed on a 3T Siemens Magnetom MRI. Two Suffolk and one Rambouillet sheep were used (average weight 60 kg and 40 kg, respectively).
Left main: no significant stenosis. LAD: proximal 60% eccentric stenosis the hemodynamic significance of which is indeterminate. RCA: Dominant: Mid 50-60% stenosis. Regional wall motion abnormality-inferolateral (this is the formal ultrasound location of a posterior wall motion abnormality).
PMID: 34775811; PMCID: PMC9075358 A bedside ultrasound was performed, shown here: Parasternal short axis view demonstrating inferior LV wall motion akinesis Apical 2 chamber view again demonstrating inferior LV wall akinesis The cath lab was not activated based on the ECG and bedside echo. J Am Heart Assoc. 2021 Dec 7;10(23):e022866.
Here are a couple shots with strain, or "speckle tracking" on ED Echo: To, me these look like anterior wall motion abnormality, but I showed them to one of our ultrasound fellows who is very interested in this. They read it as normal. She said: This is a tough one. Regional wall motion abnormality-distal septum and apex. It was stented.
During echocardiography, a transducer transmits the ultrasound beam towards the heart. Planimetry of mitral valve area can be obtained in parasternal short axis view in case of mitral stenosis. It is used in the emergency department, at bedside, in the intensive care unit as well as in the operating room.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content