This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
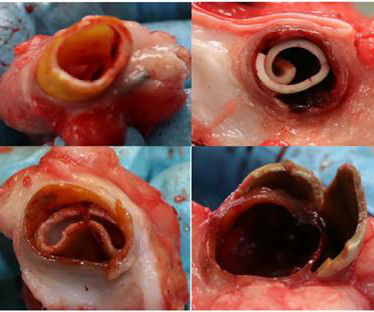
Background Subclinical leaflet thrombosis (SLT) is a common complication after transcatheter aortic valve replacement (TAVR). Methods This prospective cohort study consecutively enrolled patients with severe symptomatic aortic stenosis who underwent successful TAVR.
Transcatheter aortic valve replacement (TAVR) has become a leading treatment for aortic stenosis, but managing thromboembolic and bleeding risks post-procedure remains challenging. Subclinical leaflet thrombosis is observed in 10%20% of patients, though its clinical significance remains uncertain. Clinical valve thrombosis is rare.
The NOTION trial, a pioneering study, sought to compare the long-term clinical and bioprosthesis outcomes of Transcatheter Aortic Valve Implantation (TAVI) versus Surgical Aortic Valve Replacement (SAVR) in patients with severe aortic valve stenosis (AS) at lower surgical risk. No cases of clinical valve thrombosis were reported.
Since the pathologist does not know the original cross-sectional area of the artery or the amount of compensatory enlargement of the artery from evaluation of a single cross section of the artery at a site of stenosis, the degree of luminal narrowing of that segment cannot be determined. These are typical findings at sites of plaque rupture.
In the meta-analysis of seven randomized trials, published in JSCAI and presented at the 2024 EuroPCR conference in Paris, France, researchers compared the outcomes of 7,785 patients undergoing TAVR (a procedure that delivers a new aortic valve into the heart through a catheter) to those undergoing SAVR for severe aortic stenosis.
The LM has an irregular 30% distal stenosis, followed by an 80% ostial LAD stenosis, and total occlusion of the LAD proximally with TIMI grade 1 flow in the distal vessel. The LCX demonstrates an ostial 80% stenosis prior to the bifurcation of a large OM artery. A large Diagonal artery has subtotal occlusion proximally.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. There may be a chronic tight stenosis and a non-obstructed lesion that thrombosed.
The risk of stroke recurrence among patients with ICAD-related stroke is the highest among those with confirmed stroke and stenosis ≥70%. In fact, the 1-year recurrent stroke rate of >20% among those with stenosis >70% is one of the highest rates among common causes of stroke.
Stroke, Volume 56, Issue Suppl_1 , Page ADP36-ADP36, February 1, 2025. All patients had headache, and funduscopic examination demonstrated papilledema for all patients. All patients had headache, and funduscopic examination demonstrated papilledema for all patients.
The risk of stent thrombosis is particularly increased during the first 6 months after intervention. Key exclusion criteria included <18 or >75 years of age, contraindications to anticoagulant use, or acute venous thrombosis <3 months.
Anaphylaxis leads to plaque rupture or erosion leading to acute myocardial infarction (type II) and acute coronary stent thrombosis (type III). Emergency coronary angiography showed coronary spasm and moderate lumen stenosis in the middle segment of left anterior descending artery (LAD).
Background Arteriovenous (AV) grafts often develop severe complications of stenosis due to neointimal proliferation that occurs either at the venous anastomosis site or at the outflow receiving vein. Conclusions Almost all of the grafts occluded during the 12 months of follow up.
1-4 Surprisingly, serial angiographic studies have revealed that the plaque at the site of the culprit lesion of a future acute myocardial infarction often does not cause stenosis that, as seen on the antecedent angiogram, is sufficiently severe to limit flow. Learning Points: 1.
Coronary angiography gives a visual impression about the severity of the stenosis. But it need not imply the actual functional significance of the stenosis in terms of flow physiology. A downside of the study was that it had included lesions of 50 to 79% stenosis also. identified physiologically significant stenosis.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. elevated BP), but rather directly correlated with coronary obstruction (due to plaque rupture and thrombosis) and, potentially, stymied TIMI flow. Aortic Stenosis f.
MRA head demonstrated multifocal arterial stenosis. Repeat CTA head/neck and CT perfusion showed severe stenosis of bilateral M1 segments and left greater than right A1 segments as well as ischemic penumbra in left ACA/MCA watershed territory. After the second treatment, she had improvement in speech and motor strength.
Current guidelines recommend percutaneous coronary intervention (PCI) for significant non-infarct artery (-ies) (non-IRA) stenosis in hemodynamically stable AMI patients with MVD, either during or after successful primary PCI, within 45-days. However, deciding the timing of revascularization for non-IRA in cases of MVD is uncertain.
Notably, the LAD had multiple aneurysmal segments and areas of eccentric stenosis upto 90%.Multislice At the time of discharge, LV systolic function improved to 39% and there were no findings concerning for coronary artery thrombosis or fistula repair failure.
The angiogram showed an open artery with 95% stenosis and thrombosis and it was stented. I would expect TIMI-3 flow (normal flow, no persistent ischemia) with a culprit in the RCA (or possibly Circumflex). I would expect that a stent would be placed.
Computed tomography angiography (CTA) of the brain and neck did not show significant stenosis or occlusion. Doppler of lower extremities showed deep vein thrombosis in the left femoral vein. During admission, transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) did not reveal any source for cardioembolism.
CT angiography (CTA) of the head and neck demonstrated a nearly occlusive thrombus of the distal right M2 segment MCA as well as non‐hemodynamic stenosis of the proximal right ICA with possible underlying sidewall filling defect‐appearing lesion concerning for a posterior wall thrombus without underlying atherosclerosis at the bulb or otherwise.
History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.” Left main? 3-vessel disease?
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. This is diagnostic is inferior OMI , accompanied by inferior Q waves, and with a flat ST segment in V2 that could indicate posterior extension.
SMART 4 ( NCT04722250 ) studied patients with severe aortic stenosis and a small aortic annulus who underwent transcatheter aortic valve replacement (TAVR). The primary non-inferiority endpoint was MACCE (a composite of cardiac death, MI, ischaemic stroke, stent thrombosis, or target vessel revascularisation).
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. This is written by Willy Frick, an amazing cardiology fellow in St. He described it as "10/10" intensity, radiating across his chest from right to left.
distal stenosis or occluded small branches), and 3) nonischemic causes for myocyte injury (e.g., Coronary thrombosis or embolism can result in MINOCA, either with or without a hypercoagulable state. The diagnosis of MINOCA should exclude: 1) other overt causes for elevated troponin (e.g., pulmonary embolism, sepsis, etc.),
The cardiologist called this 20% stenosis. Furthermore, the operator worried about the patient's adherence to dual antiplatelet therapy, in which case she would be at risk for catastrophic stent thrombosis. In a large proportion of cath labs, the operator would probably have ended the case at this point.
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. As a brief review, HCM is a genetically inherited disorder that produces structural disarray in the myocardial cells. References Naidu, S.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content