This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
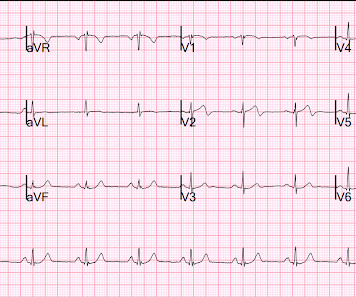
ECG in a person with persistent anginal pain for the past several hours showing significant ST segment depression anterolateral leads along with sinus tachycardia. Such a pattern is consistent with significant left main coronary artery stenosis. ST segment elevation is noted in aVR.
The LM has an irregular 30% distal stenosis, followed by an 80% ostial LAD stenosis, and total occlusion of the LAD proximally with TIMI grade 1 flow in the distal vessel. The LCX demonstrates an ostial 80% stenosis prior to the bifurcation of a large OM artery. A large Diagonal artery has subtotal occlusion proximally.
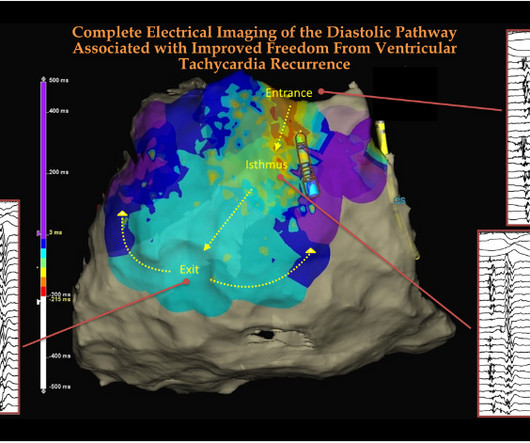
Abstract Introduction Catheter-based radiofrequency (RF) ablation is generally regarded as the standard approach for patients with ventricular tachycardia (VT) refractory to antiarrhythmic drug therapy and may be considered as a first-line approach when there is a preference to avoid these agents.
Clinical introduction A woman in her 30s, a case of rheumatic mitral stenosis status post balloon mitral valvuloplasty 15 years prior, presented to urgent care with palpitations and dyspnoea for 1 week. She was noted to be in heart failure, with hypotension and tachycardia.
This ultimately resulted in severe coronary artery occlusion, myocardial scarring and frequent episodes of ventricular tachycardia, which had a significant impact on the patient's quality of life. It is recommended that young and middle-aged patients with severe coronary artery stenosis undergo screening for embolism.
In all probability, this dilation is a form of atrial tachycardia and atrial cardiomyopathy. Spatial relationship of sites for atrial fibrillation drivers and atrial tachycardia in patients with both arrhythmias July 2017 International Journal of Cardiology 248(3) AF begets AF. Implications for electrophysiologists.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. I said I think there is a fixed stenosis in the LAD and the tachycardia and stress caused a type 2 STEMI.
The tachycardia was gone by the time paramedics arrived. He was unconscious for 8 minutes and slowly awoke in the ambulance, complaining of nausea only. First responders found him to be very tachycardic , confused, perserverating and with no memory of the event. There was tongue biting. Lightheadedness continued. Interpretation.
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. It is hard to make out P waves but you can see them best in V2, and notches in the T waves in other leads - this is a sinus tachycardia with a very long PR interval indicating first degree block.
Category 2 : An increase in myocardial oxygen demand due to tachycardia, elevated ventricular afterload (BP or aortic stenosis), or increased wall stretch (admittedly this latter is more complicated) or a decrease in oxygen supply due to hypotension, anemia, hypoxia, or a combination of all of the above. Aortic Stenosis f.
Sometimes, head up tilt test, also known in short as HUTT, is also done for the evaluation of postural orthostatic tachycardia syndrome, POTS, a condition in which there is tachycardia on standing up, without a fall in blood pressure. Transcript of the video: Head up tilt test, is usually done for the evaluation of recurrent syncope.
During active chest pain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF. Subendocardial Ischemia from another Cause ( ie, sustained tachycardia — sinus or from some other arrhythmia; shock/profound hypotension; GI bleeding; anemia; etc. ).
An EKG was repeated around midnight: By itself, this ECG is not diagnostic of anything besides sinus tachycardia, and could be called normal (although there is ST segment straightening in the anterior leads, which should always prompt suspicion). The conventional computer algorithm called “ sinus tachycardia, otherwise normal EKG ”.
This usually represents posterior OMI, but in tachycardia and especially after cardiac arrest, this could simply be demand ischemia, residual subendocardial ischemia due to the low flow state of the cardiac arrest. This prompted cath lab activation. On arrival to the ED, this ECG was recorded: What do you think? TIMI-0 flow.
A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. The aortic valve in this example also had critical stenosis by Doppler The patient continued to be hemodynamically unstable with poor cardiac output and very high LV filling pressures.
We can take a cue from the vintage clinical auscultation classes, where we ask the medical students to look for MDM (mid-diastolic murmur) in mitral stenosis in the left lateral posture in expiratory phase. How can we remember this EP lesson easily ? Reference Alexios Hadjis , Antonio Frontera. 2020;13:e008651. DOI: 10.1161/CIRCEP.120.008651
From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. McLaren : We’ve answered the first question – Sinus Tachycardia with episodic runs of wide QRS (RBBB morphology) and PVC’s.
The Y descent is shallow in tricuspid stenosis, and absent in cardiac tamponade. Right atrial hypertrophy as in tricuspid stenosis, pulmonary stenosis and pulmonary hypertension. One is ventricular tachycardia with regular retrograde activation. X descent, X prime descent and Y descent. Second is junctional tachycarida.
History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ). Anything more on history?
One clinically nonsignificant PV stenosis occurred in the VHPSD group. Compared to PFA VHPSD-PVI might ensure information on left atrial substrate allowing to target concomitant secondary tachycardias. Two tamponades occurred in the PFA while in VHPSD two pts suffered groin bleedings.
Angiography revealed a 30% nonobstructive stenosis of the mid LAD. He had multiple episodes of bradycardia and nonsustained ventricular tachycardia. There was a 70% culprit stenosis of the first obtuse marginal branch in a right dominant system. Serial high sensitivity troponin T (URL 15 ng/L) values were negative and stagnant.
Lesion on Dist RCA: 90% stenosis reduced to 0%. Thus, the very well informed physician could differentiate these ECGs from those of an LBBB patient with MI: 1) no concordance 2) no excessive discordance 3) LBBB with tachycardia, probably rate related 4) subsequent T wave inversion that, according to Shvilkin et al.,
LAD plaque with 0-25 percent stenosis. The LAD has moderate 40% ostial-proximal LAD stenosis and severe 90% mid LAD stenosis involving first diagonal branch. --The If trops are negative and there is <50% stenosis, then the patient is safe for discharge, even if the HEART score or EDACS score are elevated.
Most Type 2 OMI are due to supply-demand O2 mismatch that do NOT involve a dynamic change in the coronanry artery: 1) decreased O2 supply from (a) low blood pressure, especially in the presence of fixed coronary stenosis (b) hypoxia, (c) anemia (d) hemoglobinopathies such as CO poisoning or (e) oxidative phosphorylation problems (CN or HS) [(d) and (..)
Prior ECG available on file from 2 months before: We do not know the clinical events happening during this ECG, but there is borderline tachycardia, PVCs, and likely some evidence of subendocardial ischemia with small STDs maximal in V5-6/II, slight reciprocal STE in aVR. Normal RV, no valve stenosis or regurgitation.
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. If it is MI, is it type 1 or type 2? Is it STEMI or NonSTEMI? Is it acute persistent occlusion?
In addition to sinus tachycardia, the only abnormalities listed by the computer were "low voltage, precordial leads" and "anteroseptal infarct, old.Q This is something that is hard to teach, but with hundreds of such cases, we have taught the artificial intelligence algorithm to recognize this. 4) There is well formed J-point notching.
found that such ECG findings only represented left main ACS in 14% of such ECGs: Only 23% of patients with the aVR STE pattern had any LM disease (fewer if defined as 50% stenosis). Here is a Previous ECG for comparison: Baseline LVH Only minimal ST depression Diffuse ST depression with ST Elevation in aVR Knotts et al.
They found non-obstructive CAD, with only a 20% stenosis of OM2 and 10% RCA. That said — the heart rate is significantly faster than it was for the prior 2 tracings ( ECGs #1 and #3 ) — so there is really no way to distinguish what might represent ST-T wave changes due to tachycardia vs evolution of the patient’s underlying disorder.
Angiography : LMCA — 90-99% osteal stenosis. LCx — 50-69% stenosis of the 1st marginal branch; with 100% distal LCx occlusion. This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). The image shows the impella device in place.
Below is a still image with the red arrow indicating the subtotal LMCA stenosis. The video below shows the coronary angiography. The image quality is not the best, but you can see the subtotal occlusion of the left main artery. Pressors could gradually be tapered within 24 hours.
BACKGROUND:Varying rates of nonsustained ventricular tachycardia (NSVT) have been reported early after transcatheter pulmonary valve replacement (TPVR) with the Harmony valve, but data regarding rhythm outcomes beyond hospital discharge are limited. Circulation: Cardiovascular Interventions, Ahead of Print.
His exam was notable for tachycardia, elevated jugular venous pressure, diffuse rales, and an early 2/6 systolic murmur loudest at the cardiac apex. Severe mitral stenosis C. Forty-eight hours after initial presentation, while in the coronary care unit, he suddenly became very dyspneic. Click here to view larger image.
Methods The primary effectiveness endpoint (PEE) was 12-month freedom from documented atrial fibrillation/atrial flutter/atrial tachycardia plus freedom from acute procedural failure, nonstudy catheter failure, repeat ablation failure, direct current cardioversion (DCCV), and Class I/III antiarrhythmic drug (AAD) failure.
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
pre-existing, stable atherosclerosis) amidst any state of global duress – to include hypertension, hypoxia, tachycardia, hypotension, sepsis, and GI bleed, for example. Advanced multi-vessel disease was found with stents deployed to the mid-LCx (80% stenosis), D1 (90% stensosis), and the pLAD (95% stenosis).
Here is another proven left main occlusion in a young woman who presented with sudden pulmonary edema, had this ECG recorded, then arrested and was resuscitated after 30 minutes of CPR: This has sinus tachycardia with RBBB and LAFB, and STE in V2-V6 as well as I, aVL This pattern could just as easily be seen in LAD occlusion. TIMI 0/1 flow).(61,62)
Although the shock is no doubt partly a result of poor pump function, with low stroke volume, especially of the RV, it should be compensated for by tachycardia. Cardiac output is stroke volume x rate, so this patient needs a higher heart rate. This is a perfect indication for atropine. He was successfully stented.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. However, there is also significant tachycardia , with heart rate of 116, and known hypoxia. Smith : "decompensation" of aortic stenosis might have initiated this entire cascade.
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. heart auscultation (aortic stenosis); c.
Right from the days we entered medical schools, severe mitral stenosis was defined by less than 1 cm² MVO by echocardiography. The bottom line is, we should not miss a functionally significant mitral stenosis, strictly adhering to the anatomical 1 cm² cut-off. There is something called low gradient severe MS (as in aortic stenosis).
August 2024 Approvals Minima Stent System (P240003) (Approval Date: August 28, 2024) The Minima Stent System is an expandable cobalt-chromium metal mesh tube to reopen blood vessels in neonates, infants, and children with Coarctation of the Aorta and Pulmonary Artery Stenosis, specifically designed to expand as younger patients grow.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content