This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
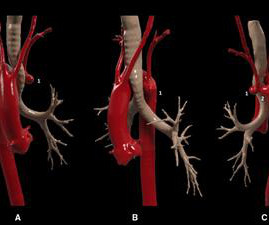
In this case, we present a symptomatic patient with a Kommerell's diverticulum and a left aberrant subclavian artery complicated by proximal stenosis and poststenotic aneurysm.
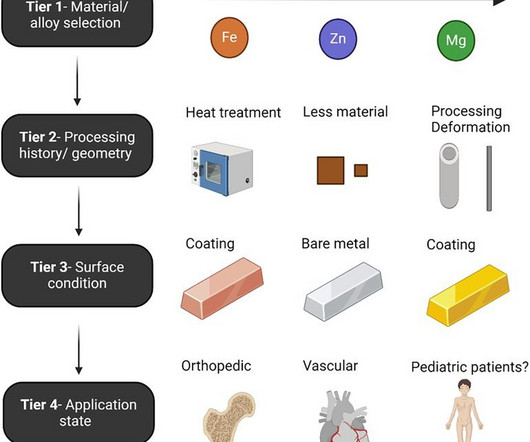
The past five years have yielded impressive advancements in fully absorbable metal stent technology. The desired ultimate ability for such devices to treat a vascular stenosis without long-term device-related complications or impeding future treatment continues to evoke excitement in clinicians and engineers alike.
Stroke, Volume 56, Issue Suppl_1 , Page ADP36-ADP36, February 1, 2025. All patients had headache, and funduscopic examination demonstrated papilledema for all patients. All patients had headache, and funduscopic examination demonstrated papilledema for all patients. Additional randomized and controlled clinical research is deserved.
The goal of the DCB-BIF trial was to assess the efficacy of drug-coated balloon (DCB) angioplasty of residual side branch stenosis in coronary bifurcation lesions treated with a provisional stenting strategy.
Some of the late-breaking topics that will be covered include transcatheter aortic valve replacement (TAVR), peripheral artery disease (PAD), and pulmonary embolism (PE): Impact of Age on Procedural Timing for Asymptomatic Severe Aortic Stenosis: Results from the Early TAVR Trial The PERFORMANCE II Trial: A Prospective Multicenter Single Arm Investigation (..)
The stenosis was treated with a stent. years later he presented with an in-stent restenosis that was successfully treated with a stent-in-stent strategy. Conclusion Our case demonstrates stenting as a viable alternative strategy with potentiallyfavorable long-term outcome.
Stent performance was assessed.ResultsWe identified 28 patients (67.8% Percentage of stenosis was 50% (IQR, 36%58%). The procedures mostly used 7 Fr sheaths for stents on 6, 7, and 8 mm balloons and 8 Fr sheaths for 9, 10, 12 mm balloons. Median stent expansion percentage was 95% (IQR, 90%96%). kg (IQR, 9.116.4).
This comprehensive literature review focuses on acute stroke related to intracranial atherosclerotic stenosis (ICAS), with an emphasis on ICAS-large vessel occlusion. Herein, we focus on current management strategies for ICAS-large vessel occlusion discussed, including the use of perfusion imaging, endovascular therapy, and stenting.
Intracranial atherosclerotic stenosis is a leading cause of stroke with a significant risk of recurrent ischemic events despite aggressive medical management. However, 3 percutaneous angioplasty and stenting randomized trials showed negative or neutral results. Stroke, Volume 56, Issue 4 , Page e114-e118, April 1, 2025.
To observe the occurrence of related complications after self-expandable metallic (SEM) airway stents implantation with different diameters at different time points, and to provide theoretical basis for the op.
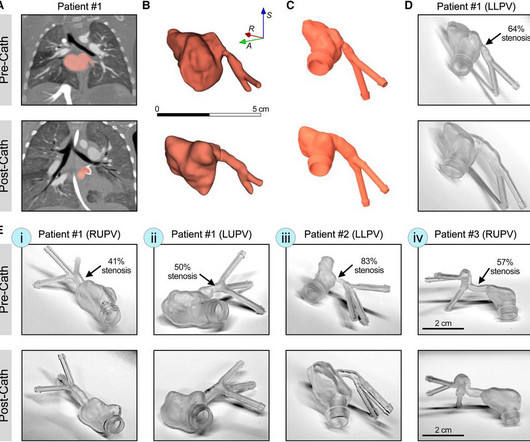
IntroductionPrimary pulmonary vein stenosis (PVS) is a rare congenital heart disease that proves to be a clinical challenge due to the rapidly progressive disease course and high rates of treatment complications.
Asymptomatic high-grade carotid stenosis is an important therapeutic target for stroke prevention. Since then, transfemoral/transradial carotid stenting and transcarotid artery revascularization have emerged as alternatives to endarterectomy for revascularization.
Introduction:Medical therapy and endovascular therapy for intracranial atherosclerotic disease (ICAD) have evolved over the past two decades with improved medical therapy benchmarks, and improved techniques and patient selection for stenting.
Logistic regression was used to assess the association between LVEF1 and coronary artery stenosis, and linear regression identified factors linked to postintervention LVEF1 improvement. LVEF1 was independently associated with coronary artery stenosis 50% or 70%. for predicting coronary artery stenosis 70%.
Background:In stroke patients undergoing EVT, angioplasty and stenting (A&S) has been described as a bailout technique when thrombectomy fails or intracranial stenosis is suspected. The stent-retriever was re-sheathed into the microcatheter before retrieval. Further prospective data is warranted.
IntroductionDrug‐eluting stent (DES) use in symptomatic intracranial atherosclerosis disease (ICAD) has been described in the literature using different guiding and distal access catheters. Decision was made to deploy a drug eluting stent into the stenosed M1 segment. No tPA was given low NIHSS and resolution of symptoms.
The objective of our study is to identify factors associated with SBIs following middle cerebral artery (MCA) stenting or balloon angioplasty.Methods:We retrospectively reviewed patients who underwent MCA stenting or balloon angioplasty, including those with symptomatic, atherosclerotic MCA stenosis of 50%. 14.74], p=0.012).
IntroductionVertebral artery stenting represents a viable option in treating symptomatic vertebral artery atherosclerotic stenosis. We included articles reporting patients > 18 years old with symptomatic extracranial vertebral artery stenoses due to atherosclerosis treated with stenting (with or without angioplasty).
Recent research has identified venous sinus stenosis as a cause of IIH, a common treatment of which is venous stenting and angioplasty. An adverse event of this procedure is in‐stentstenosis (ISS), due to either neointimal hyperplasia or hypersensitivity to an element in the stent.
OBJECTIVECarotid artery stenting for heavily calcified lesions is challenging for interventionists. They had dense calcifications at the lesions, stenosis rates of 95% (near occlusion) and 86% according to the North American Symptomatic Carotid Endarterectomy Trial criteria, and calcification arcs of 270° and 360°, respectively.
We defined high-risk post-EVT stenosis as any stenosis with 50% lumen stenosis, associated dissection, re-occlusion during thrombectomy, and severe residual luminal irregularity. Conclusions:Eptifibatide use is associated with lower re-occlusion rates in patients with residual high-risk stenosis after EVT.
Rescue treatment with stenting, balloon angioplasty, and/or intraarterial thrombolysis or antiplatelets are often required to treat the underlying stenosis. 4 Recent literature has reported clinical benefits associated with rescue stenting in the setting of ICAD‐related MT‐refractory strokes.5
The clinical impact of correct assessment of coronary artery stenosis in AF is especially high, due to the antithrombotic therapy imposed by both AF and coronary stenting. Until recently, an in‐depth characterization of coronary microcirculation in AF was lacking.
BACKGROUND:Carotid artery stenting (CAS) is an alternative treatment for patients with carotid artery stenosis who are not eligible for carotid endarterectomy. Stroke, Ahead of Print. Dual antiplatelet therapy (DAPT) after CAS aims to prevent ischemic stroke. However, its optimal duration remains unclear.
In this hyperacute emergent clinical situation, covered stents have been considered as a primary measure to prevent further serious arterial events. A fabric-based covered graft stents yield poor clinical outcomes. Both CT and angiography revealed no instances of thrombotic occlusion or in-stent restenosis (% diameter stenosis: 5.7
1 To date, interventional treatment of coronary artery disease with drug-eluting stents has been able to establish flow angiographically. 2 “For many years, it was thought that caging of the vessel with stents was the main driver for annual increasing non-plateauing event rates. of the U.S. population. JACC 2020. 5 Saito S, et al.
Introduction:Traditional endovascular treatment for acutely symptomatic intracranial atherosclerotic disease (ICAD) includes balloon angioplasty and stenting. The Tenzing was slowly inserted across the ICAD stenosis in each case under roadmap fluoroscopic guidance. Stenosis location was: 1 ICA, 7 M1, 4 M2, 2 vertebral.
PR was calculated as the ratio of proximal to distal pressure at the stenosis site, indicating post-stenosis blood flow. Arterial stenosis severity was categorized using the WASIDMethod:50%-69% for moderate and 70%-99% for severe. frequency was significantly higher in severe compared to moderate stenosis (P=0.01).
Baseline angiograms were reviewed to assess the presence or absence of intracranial stenosis lesions (IS+ Vs IS-) different than the target occlusion. Further research is warranted to explore the diagnostic value of multiple intracranial stenosis in patients undergoing mechanical thrombectomy. minutes; p=0.018). Vs 3; p=0.036).Conclusions:Our
Stenosis of the external carotid artery in such patients can be a source of atheroembolism or hypoperfusion. We describe a case of external carotid stenting with carotid stump coil occlusion.MethodsWe present a case report.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This was stented with a 2.25 x 38mm stent, post dilated with a 2.75mm balloon proximally.
Transcatheter aortic valve replacement (TAVR) is the standard treatment for severe aortic stenosis, but post-TAVR leaflet thrombus, identified by hypoattenuated leaflet thickening (HALT), poses potential risks like cerebral thromboembolic events. Perivalvular thrombus has also been reported. Specifically, 14.2% had perivalvular thrombus.
Angiogram: Widely patent RCA and LAD stents. Culprit Lesion: Angiographically indeterminate 50% stenosis in the proximal OM2 was assessed further with instantaneous wave free ratio (iFR) of 0.96, which is normal (see below for description of iFR*). Therefore, no stent was placed. (No He was treated with aspirin and heparin.
3) Rescue stenting (RS) in these patients has shown promising rates of recanalization and better outcomes in preliminary studies. Therefore, rescue stenting can be considered as a safe and viable option in these patients. 1, 2)These patients are also more likely to experience poor functional outcomes. (3)
Purpose:Since the balloon protection device became unavailable in Japan three years ago, the DWI-positive rate after carotid artery stenting (CAS) has increased. Symptomatic stenosis (63.9% Stroke, Volume 55, Issue Suppl_1 , Page ATMP68-ATMP68, February 1, 2024. vs. 94.7%, p<0.05) was more common in the with-POWER group.
BACKGROUND:In patients with post-thrombotic syndrome, stent recanalization of iliofemoral veins or the inferior vena cava can restore venous patency and improve functional outcomes. The risk of stent thrombosis is particularly increased during the first 6 months after intervention.
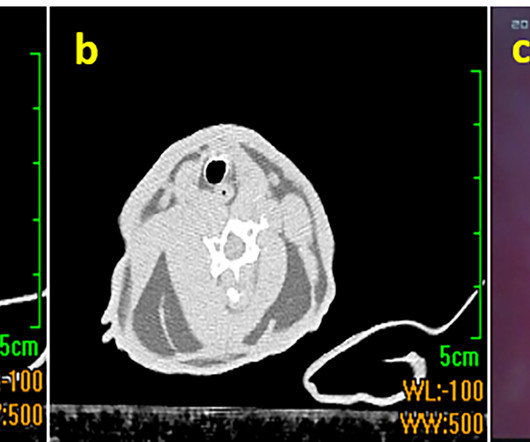
3% sodium alginate solution was cast into a stenosis mold and crosslinked in a 40% calcium chloride. After angioplasty (Gateway PTA Balloon Catheter 3.5x20mm, Boston Scientific) and stenting (Wingspan 2.5mmx15mm, Stryker) were performed the residual stenosis was <10% (Figure 1).
His disease included 70% prox LAD, 80% distal LAD, 10% in-stentstenosis in the distal LCX, 70% OM1, 70% OM2, and 60% prox RCA. Triage ECG: It was interpreted as lateral STEMI, and he was sent to the cath lab, where the angiogram showed unchanged CAD from known prior, with no acute culprit. Three troponins were undetectable.
Background:Persistent hypotension after carotid artery stenting (CAS) can lead to adverse outcomes, prolong length of stay (LOS), and increase hospital costs. A relation between decline of norepinephrine after stenting and persistent hypotension supports the role of catecholamine in BP control.
Background:Hyperperfusion phenomenon (HPP) constitutes a significant risk factor for adverse outcomes following carotid artery stenting (CAS). Stroke, Volume 56, Issue Suppl_1 , Page ATP178-ATP178, February 1, 2025. Currently, the sole method for evaluating the risk of HPP post-CAS is the invasive acetazolamide (ACZ) challenge test.
IVUS Measurements Measurements include the measurement of lumen, plaque, calcium, remodeling, stent length and volumetric measurements. In the geometry, the size of the plaque, its relationship to luminal stenosis, arterial remodeling and eccentricity can be evaluated. IVUS can also delineate intramural hematoma and dissection.
Background:Hemodynamic evaluation is crucial in assessing stroke risk in patients with symptomatic intracranial atherosclerotic stenosis (sICAS). Stroke, Volume 56, Issue Suppl_1 , Page AWP286-AWP286, February 1, 2025. before PTAS. before PTAS.
Background:Postoperative complication rates of carotid endarterectomy (CEA) and carotid artery stenting (CAS) for carotid artery stenosis are recommended to be maintained below a certain threshold. Stroke, Volume 56, Issue Suppl_1 , Page ATP128-ATP128, February 1, 2025.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content