This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
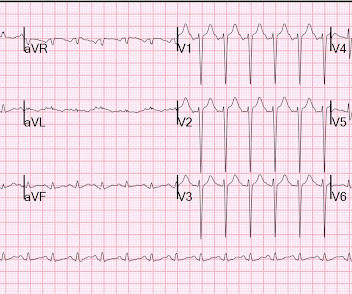
There is LBBB with concordant ST elevation in II and aVF (inferior STEMI) and V6 (lateral STEMI); also concordant ST depression in V2 and V3 (Posterior STEMI). The physician (one of our fine EM residents) caring for the patient did an immediate bedside ultrasound. He complained of chest pain. This ECG was recorded.
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardial infarction (STEMI). We present the case of a man in his 50s, admitted with cardiac arrest secondary to inferolateral STEMI.
This is all suggestive of posterior STEMI, but not definitely diagnostic. mm in only one posterior lead is highly sensitive and specific for posterior STEMI). I performed a bedside cardiac ultrasound and the posterior wall appeared to be contracting and shortening normally. The ECG normalized overnight. Maximum troponin was 2.1
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. At first glance, it seems the patient is having a STEMI. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock.
We did a bedside cardiac ultrasound. This is as clear a STEMI as you can get. So this is classic inferoposterior STEMI on the ECG but is NOT acute coronary syndrome! The ECG and ultrasound could not have been differentiated from acute plaque rupture with occlusion of the RCA. 3 points gets you an MI by Sgarbossa.
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. He had diffuse crackles on exam and B-lines on chest ultrasound, and chest x-ray also confirmed pulmonary edema. Is this acute STEMI? Is this an acute STEMI? -- Unlikely!
The following ECG was recorded: There is an obvious acute inferior STEMI. Whenever there is inferior STEMI, one should think about Right Ventricular STEMI (RVMI). As 85% of inferior STEMI are due to RCA occlusion [the rest due to occlusion of a "dominant" circumflex (i.e., and STE in lead III > STE in lead II.
The conventional machine algorithm interpreted this ECG as STEMI. Answer : Bedside ultrasound! Smith : RV infarct may also have this appearance on ultrasound. So hypoxia without B lines on lung ultrasound strongly weights toward PE. So hypoxia without B lines on lung ultrasound strongly weights toward PE.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. Troponin was elevated and no “STEMI” was seen on the EKG, so if it is acute MI, then “NSTEMI” is the diagnosis (however flawed), not a pathology on the differential.
She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI. Gallbladder ultrasound was negative for stones. Chest x-ray was normal.
The computer read Anterior STEMI along with RBBB. I would activate the cath lab based on this and the clinical presentation, but I do NOT see any evidence of anterior STEMI The patient arrived in the ED and had this ECG: The T-waves are now less hyperacute, but ST Elevation remains. Here is his prehospital ECG: What do you think?
This case was posted on the [link] ultrasound site, of which this ECG blog is a part. I refer you to the video case presentation by one of my colleagues, Dr. Rob Reardon (who has, by the way, a fantastic collection of ED ultrasound cases). In this case, the ECG never mimicked a STEMI.
The problem is difficult to study because angiographic visualization of arteries is not perfect, and not all angiograms employ intravascular ultrasound (IVUS) to assess for unseen plaque or for plaque whose rupture and ulceration cannot be seen on angiogram. Thus, intracoronary imaging modalities are crucial in this setting. From Gue at al.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Bedside cardiac ultrasound with no obvious wall motion abnormalities. . — He had a previous ECG on file: Proving the findings are new The cath lab was activated. He was given aspirin and sublingual nitro and the pain resolved.
This was sent by a recent ultrasound fellow, asking for my ECG diagnosis. However, there are morphologies of Takotsubo that cannot be distinguished from STEMI. Takotsubo This looks like and infero-posterior STEMI, but the QT is bizarrely long. There is ST elevation in I, II, III, aVF, V2, V3, V4, V5, and V6.
This meets "STEMI criteria" However, there is very high voltage, with a very deep S-wave in V2 and tall R-wave in V4. The morphology is not right for STEMI. My interpretation: LVH with secondary ST-T abnormalities, exaggerated by stress, not a STEMI. This is very good evidence that the ST elevation is not due to STEMI.
Bedside ultrasound with no apparent wall motion abnormalities, no pericardial effusion, no right heart strain. Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). Labs ordered but not yet drawn.
A bedside ultrasound was done, with dozens of clips, and was even done with Speckle Tracking. Because we are hypnotized the STEMI paradigm. "If If there is no STEMI, there is no emergent problem and the patient can wait." It was not a STEMI) 1. To me, this looks like pulmonary edema. Here are a few clips.
There is an obvious inferior posterior STEMI(+) OMI. Case continued A bedside ultrasound showed diminished LV EF and of course bradycardia. Results Of 149 patients with inferior STEMI , 43 (29%) had RVMI and 106 (71%) did not. What is the atrial activity? Is it sinus arrest with junctional escape? How would one tell?
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Takotsubo is a sudden event, not one with crescendo angina.
Could this be Septal STEMI (STE in V1 and aVR, with reciprocal ST depression in V4-V6?), In Septal STEMI , transmural ischemia of the septum is recorded by the overlying lead V1 as ST Elevation. Lead III is also on the right and might manifest ST Elevation in Septal STEMI. with ADDED STE in III?
EMS recorded these ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 Here are a couple shots with strain, or "speckle tracking" on ED Echo: To, me these look like anterior wall motion abnormality, but I showed them to one of our ultrasound fellows who is very interested in this. She called 911.
Prehospital Conventional algorithm interpretation: ANTERIOR INFARCT, STEMI Transformed ECG by PM Cardio: PM Cardio AI Bot interpretation: OMI with High Confidence What do you think? On arrival, lung ultrasound confirmed pulmonary edema (B lines). This is proximal LAD Occlusion until proven otherwise.
A bedside ultrasound revealed a possible anterior wall motion abnormality. They may be the only remaining clue to a reperfused LAD occlusion. Today the discomfort is associated with multiple episodes of vomiting and it is unremittant. The following EKG was obtained and hyperkalemia was diagnosed. The K returned at 2.9
This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI. I believe the latter (type II STEMI) is most likely.
Given her risk factors (HTN, HLD, ESRD from diabetes) I decided to obtain a broad cardiac workup for the patient: serial ECGs, labs, serial troponins, CXR and bedside cardiac ultrasound. Ultrasounds can be very helpful in guiding your diagnostic pathway: location of WMA on US led to obtaining posterior leads.
Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. But what we truly care about is coronary occlusion, for which STEMI is just a surrogate that is only about 75% sensitive for occlusion. Some are STEMI-equivalents.
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Similarly, STEMI guidelines call for urgent angiography for refractory ischemia or electrical/hemodynamic instability, regardless of ECG findings. On arrival, GCS was 13 and the patient complained of ongoing chest pain.
On intravascular ultrasound (IVUS), the mid RCA plaque was described as "cratered, inflamed, and bulky," and the OM plaque was described as "bulky with evidence of inflammation and probably ulceration." From angiography, it is not clear what the culprit is. The ECG changes were inferior, posterior, and lateral.
An emergency cardiac ultrasound could be very useful. The upright portion of the T-wave in aVF is very large compared to the QRS size. These findings mandate that the patient at least get serial ECGs. If these remain unchanged, then serial troponins.
When the ST vector is primarily posterior, the diagnosis is usually posterior STEMI. ST depression maximal in V5 and V6 cannot be reciprocal to subepicardial, transmural ischemia under aVR because, as stated above, there is no ventricular myocardium beneath that lead, no STEMI under aVR. I just read Ken's comments before publishing.
A bedside cardiac ultrasound was normal. Is there STEMI? This case was sent by Dr Avinash Krishnamurthy, a fine emergency medicine resident from Australia Cairns base hospital Case : An adolescent male had a mechanical fall and injured his left shoulder and arm. His chest was tender. He wrote: "ECG 1 - shows wide ???IVCD What is it?
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI. QTc is the computer measurement. 100% LAD occlusion.
This was a point of care ultrasound, not a bubble contrast echo. What do you think the echocardiogram shows? First trop I returns at 1.5. POCUS Echo: POCUS Echo with no wall motion abnormality and normal ejection fraction. Sensitivity of POCUS even for definite wall motion abnormalities is far from perfect. Is this OMI?
Smith comment: This patient did not have a bedside ultrasound. Had one been done, it would have shown a feature that is apparent on this ultrasound (however, this patient's LV function would not be as good as in this clip): This is recorded with the LV on the right. In fact, bedside ultrasound might even find severe aortic stenosis.
Two thirds of MINOCA cases are due to atherosclerotic causes One way to prove the diagnosis in this case would have been with intravascular imaging such as optical coherence tomography (OCT) or intravascular ultrasound (IVUS). Fortunately, that is exactly what happened.
On arrival, the patient was in shock, was intubated, and had an immediate cardiac ultrasound. What does a heart look like on ultrasound when the EKG looks like that? Here you go: It's not the world's greatest cardiac ultrasound video, but it does appear to show poor function and low volume. They transported to the ED.
Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. Regional wall motion abnormality-inferolateral (this is the formal ultrasound location of a posterior wall motion abnormality). After return from CT, the patient's pain was severe again. 2022.08.750 Section 5.2.2,
A recent study found that SCAD causes almost 20% of STEMI in young women. Often, intravascular ultrasound or intravascular optical coherence tomography is requeried to make the diagnosis. examined SCAD presenting as STEMI (unlike Hassan et al. Type 2 is more difficult to appreciate on angiography than type 1. Lobo et al.
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 To, me these look like anterior wall motion abnormality, but I showed them to one of our ultrasound fellows who is very interested in this. She was having a transient STEMI, briefly. She called 911.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content