This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI.
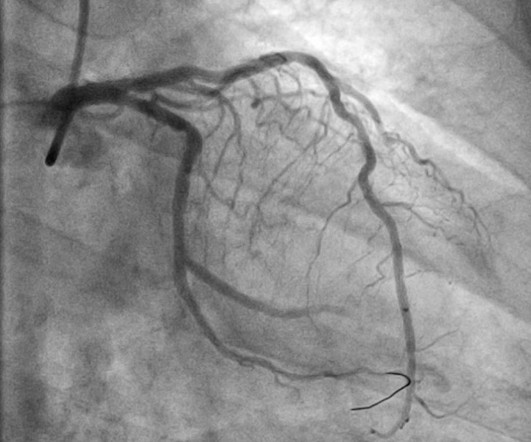
Triage ECG: It was interpreted as lateral STEMI, and he was sent to the cath lab, where the angiogram showed unchanged CAD from known prior, with no acute culprit. His disease included 70% prox LAD, 80% distal LAD, 10% in-stentstenosis in the distal LCX, 70% OM1, 70% OM2, and 60% prox RCA. Three troponins were undetectable.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. Most large STEMI have peak troponin I in the 20.0 This was stented with a 2.25 Next trop in AM.
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria. Two stents were placed with resultant TIMI 3 flow. What do you think? Of course not.
The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. Or is it a very tight stenosis that does not allow enough flow to perfuse myocardium that has a high oxygen demand from severely elevated BP?
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Angiogram findings included: 95% mid RCA stenosis with occluded distal right PDA secondary to thrombus (peristent OMI). At this point — a STEMI was diagnosed, and cardiac cath with PCI was performed.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The two cases were considered: Patient 1 was recognized by the ED provider and the cardiologist as having resolved “STEMI”. It was stented.
I would expect that a stent would be placed. The angiogram showed an open artery with 95% stenosis and thrombosis and it was stented. Quiz : What percent of full blown STEMI have an open artery with normal flow at angiogram? In the meantime, a lot of myocardium is lost. They were interpreted as completely NORMAL!!
Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. Here is the angiogram: --Culprit is 100% stenosis in the proximal RCA. Here is the angiogram: --Culprit is 100% stenosis in the proximal RCA. (It
This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria. You can find the variables used to calculate the value on MD calc here: [link] Utilizing Dr. Smith’s Subtle Anterior STEMI Calculator (4-Variable), the value is greater than 18.2 The culprit mid LAD lesion was stented.
RBBB in acute STEMI has a very high mortality. Angiography revealed a very tight LAD stenosis with some flow (confirming the reperfusion that we see on the ECG). A stent was placed, and the patient had an excellent outcome with no wall motion abnormality. But here there is a large degree of ST elevation in V2-V6, I, and aVL.
The LAD has diffuse disease with a few areas of moderate stenosis but no flow-limiting lesions. On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions. OM before and after, arrow indicating stented region.
It was opened and stented. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. But what we truly care about is coronary occlusion, for which STEMI is just a surrogate that is only about 75% sensitive for occlusion. RCA: dominant.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. So there is pathologic ST elevation here, consistent with anterolateral STEMI. Called 911.
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. The troponin I returned at 4.1 ng/mL (ULN = 0.030 ng/mL) , diagnostic of myocardial injury. mm STE in one lead.
There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. The case was reviewed by all parties, and it was stated correctly that the ECG does not meet the STEMI criteria. The LAD lesion was acute and required 3 stents to restore flow.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
LAD plaque with 0-25 percent stenosis. Later, she developed chest pain again, and had this ECG recorded: Obvious Anterior OMI that is also a STEMI Coronary angiogram- --Right dominant coronary artery system --The left main artery was normal in appearance and free of obstructive disease. --The A CT Coronary angiogram was ordered.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. The image on the left shows the LAD before intervention, and the red circled portion on the right indicates the stented region.
At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). The red arrow points to a 90% stenosis in the proximal segment of the LAD. RAO Caudal View Post PCI This is the RAO Caudal view after thrombectomy and stent placement. At 1605, another repeat troponin resulted at 5.271 ng/mL.
EMS recorded these ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. It was stented. She called 911. mm at the J-point, relative to the PQ junction.
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. A stent was placed. When the patient had chest pain, prior to nitroglycerine, what do you think the ECG showed ? de Zwaan C., Wellens H.J.J.,
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. It was stented. If you want to understand aVR, read this.]
The STD in V2-V4 is almost certainly reciprocal STD, reciprocal to STEMI in the posterior wall; this is evident because it is maximal in V2-V4, not in V4-V6. There is evidence that de Winter's T-waves really represent a tiny trickle of blood through the thrombotic stenosis. Both were stented. mm ST depression in aVL.
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI. Angiogram showed a critical LAD thrombotic stenosis.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin. Pre-intervention.
There is ventricular hypertrophy in the absence of abnormal loading conditions, such as aortic stenosis, or hypertension, for example – of which the most common variant is Asymmetric Septal Hypertrophy. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital.
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. He was successfully stented.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. See these posts for Wellens' mimics: Pseudo-Wellens' Syndrome due to Left Ventricular Hypertrophy (LVH) Anterior STEMI? Am Heart J.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. In the setting of prior stenting and reduced left ventricular ejection fraction, would pursue a heart team revascularization approach Syntax score 28.5, This alone could be due to LVH, but V4 could NOT be due to LVH.
It was opened and stented with resulting TIMI-3 (normal) flow. The stent to LCX is patent. OM1 is occluded and OM2 has 60% stenosis. Her RCA is a medium caliber vessel with tandem, at least moderate stenosis in the mid segment. Marked acute STEMI changes in no less than 4 lateral leads. A balloon pump was placed.
STEMI was activated and the patient went to Cath on arrival. Advanced multi-vessel disease was found with stents deployed to the mid-LCx (80% stenosis), D1 (90% stensosis), and the pLAD (95% stenosis). Of these, the pLAD was determined to be the acute culprit.
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 She was having a transient STEMI, briefly. It did not progress to full STEMI with loss of the anterior wall, as in this case. It was stented. She called 911. Learning Points : 1. See this case.
This can only be due to STEMI. Here I annotate it: This shows 100% occluded circumflex (red arrow) and a 90% stenosis of the LAD (Yellow arrow). The LAD was thought to be not thrombotic, but a chronic tight stenosis. The LAD was thought to be not thrombotic, but a chronic tight stenosis. I said "activate the cath lab."
But it does not meet the ridiculous "STEMI criteria" since there is not 1 mm of STE in any lead. Here is the angiogram: Very tight stenosis in circumflex, but with TIMI-3 flow, thanks to thrombolytics. Here is the circumflex after stenting: Wide open The cardiologist called Dr. Lufkin back and said "Great call!!"
The is very small STE in III and aVF which do not meet STEMI criteria, hyperacute T waves, reciprocal TWI in aVL, and maximal STD in V2-V3 showing posterior OMI. The cath lab was activated despite lack of STEMI criteria, around 2 am in the morning. 33% of STEMI are reperfused by the time of angiography. Very frustrating.
The therapeutics of coronary stenosis has become a technogical wonder, interwoven with statistical wordplay in the last few decades. He is a STEMI patient (1 year old) with mild LV dysfunction and thinning of IVS and anterior wall. OMT often turns out to be the savior of stents, but the latter ruthlessly steals the credit.
At 1210, the case was discussed with a cardiologist at a PCI capable facility, who accepted the patient for transfer, noting the ST depression in anterior leads as consistent with ischemia but not a STEMI. The proximal and mid LAD stenoses were stented and the OM 2 was left alone. Subendocardial ischemia does not localize.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". First obtuse marginal also had an 80% stenosis and was stented. Pt received 324 ASA and 2 sprays of nitro with improvement. Cath lab was activated by EMS and transported emergent." Pain was decreased to 2/10.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















































Let's personalize your content