This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
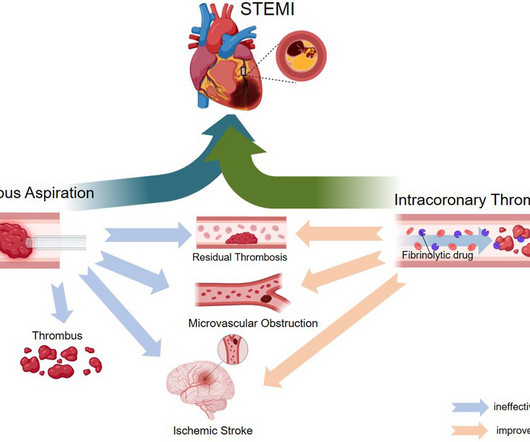
ST-elevation myocardial infarction (STEMI) is a critical cardiovascular emergency characterized by acute coronary artery occlusion and subsequent myocardial injury. The pathophysiology of MVO is systematically reviewed, followed by an evaluation of clinical studies on thrombus aspiration and intracoronary thrombolysis in STEMI management.
Jesse McLaren illustrates the paradigm shift from STEMI to Occlusion MI (OMI) through 9 cases, and drives home the points that if there is STEMI criteria, consider false positives (eg. secondary and proportional to LVH or BER); if there is no STEMI criteria, consider false negatives and look for other signs of occlusion (eg.
ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ). . = R elated E CG B log P osts to Today’s Case : ECG Blog #205 — Reviews my S ystematic A pproach to 12-lead ECG Interpretation.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
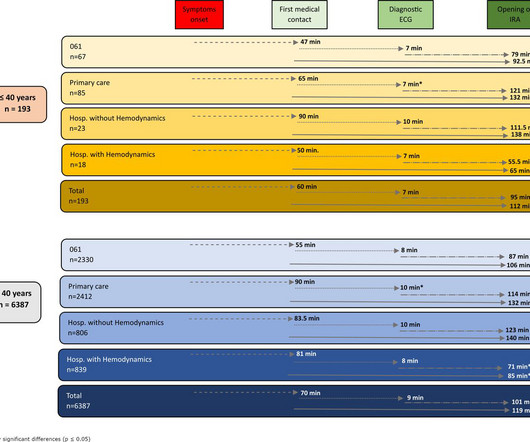
Introduction ST-elevation myocardial infarction (STEMI) is one of the most prevalent presentations in young patients. Methods A retrospective, multicentre cohort study was carried out in 6799 patients diagnosed with STEMI. to 1.54) (p<0.042).
This randomized clinical trial investigates if prehospital pulse-dose glucocorticoid treatment has a cardioprotective effect in patients with ST-segment elevation myocardial infarction (STEMI).
How can we use the awareness of complications to identify false positive STEMI and Occlusion MI that doesn’t meet classic STEMI criteria, and consider specific treatment? The post ECG Cases 41 – STEMI, Occlusion MI Complications appeared first on Emergency Medicine Cases.
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
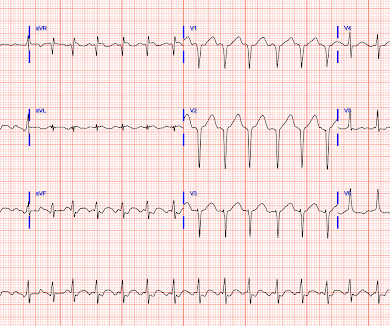
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
What is the impact of complete revascularization versus culprit-only revascularization on outcomes in older patients with ST-segment elevation myocardial infarction (STEMI) and non–ST-segment elevation myocardial infarction (NSTEMI)?
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. It is a mass delusion.
This narrative review aims to evaluate strategies for reducing door-to-balloon (D2B) time in ST-elevation myocardial infarction (STEMI) patients, focusing on pre-hospital, in-hospital, and technological innovations, as well as addressing challenges to ensure sustainability.
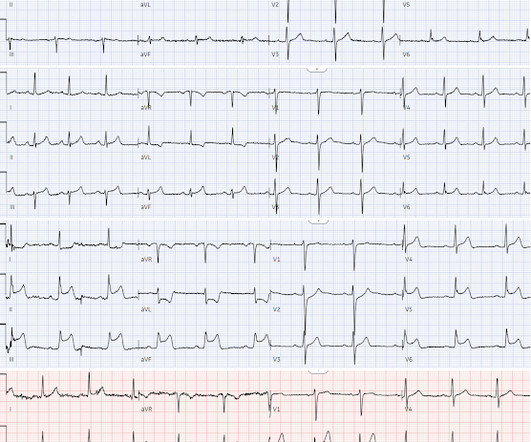
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
The lymphocyte to C-reactive protein ratio (LCR) has been established as be a reliable inflammation marker and is associated with the prognosis of patients with ST-segment elevation myocardial infarction (STEMI). ConclusionLower LCR is independently associated with the risk of LVT in patients with STEMI after pPCI.
To support EM Cases, please consider a donation here: [link] The post EM Quick Hits 57 – HIV Diagnosis, Failed Paradigm of STEMI Criteria, Poisoned Patient Airway Management, Spontaneous Bacterial Peritonitis, DIY Investments appeared first on Emergency Medicine Cases.
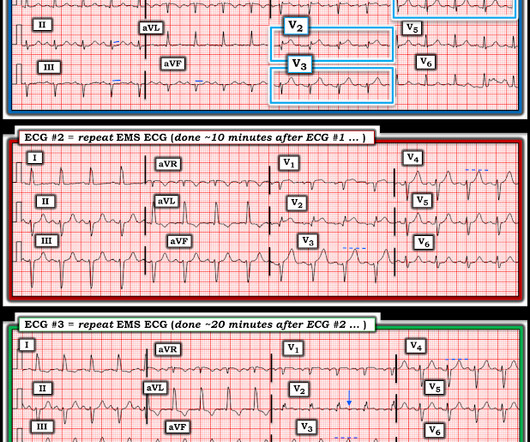
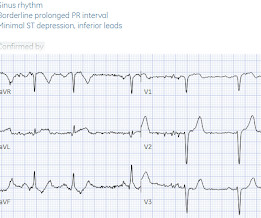
The Patient: A 60-year-old man at work. He experienced a sudden onset of substernal chest pain, nausea & vomiting, and dizziness. He states the pain is a 5 on 1-10 scale. No cardiac history or current medications. The ECGs: The first ECG , taken at 12:30:05, shows a sinus rhythm with ventricular bigeminy.
(MedPage Today) -- ATLANTA -- Routine use of the Impella CP microaxial flow pump significantly improved survival in patients with infarct-related cardiogenic shock, the randomized DanGer Shock trial showed. In more than 350 patients receiving.
Replace STEMI/NSTEMI with OMI/NOMI and AI in the ECG Diagnosis of OMI If you want to find it in the future, you can always find it at the banner above: I gave this Grand Rounds to UC Riverside a couple weeks ago. It is my most up to date lecture on OMI NOMI and Use of AI, especially the Queen of Hearts, in the Diagnosis of Occlusion MI.
What are long-term clinical benefits of complete versus culprit-only revascularization among ST-segment elevation myocardial infarction (STEMI) patients aged ≥75 years?
The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. For this reason, ECGs need first to be interpreted in isolation, and then applied to the patient. Could this false positive cath lab activation been prevented?
He discusses how using multiple OMI findings such as acute Q wave, subtle STE, reciprocal STD, hyperacute T waves, and reciprocal TWI to contribute to your overall impression, can double the sensitivity of STEMI criteria for acute coronary occlusion.
What is the safety and effectiveness of P2Y12 inhibitor pretreatment in patients transferred for primary percutaneous coronary intervention (PPCI) within a regional ST-segment elevation myocardial infarction (STEMI) network?
Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen.
Introduction ST-segment elevation myocardial infarction (STEMI) diagnosis is based on a clinical presentation and ST-segment elevation (STE) in at least two consecutive leads. 1 This paradox stems from the incorporation bias and feedback sanction bias detailed in subsequent paragraphs.
What are the outcomes of bivalirudin vs. heparin anticoagulation during percutaneous coronary intervention (PCI) in patients with ST-segment elevation myocardial infarction (STEMI)?
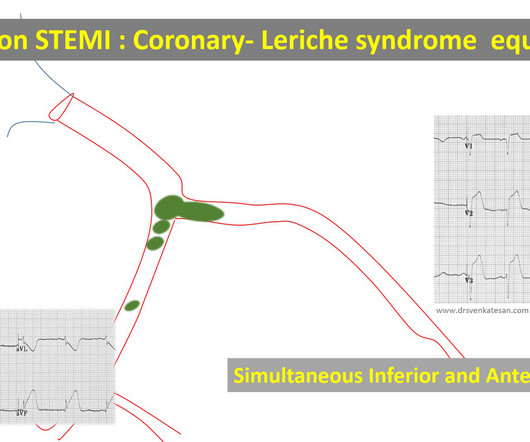
True bifurcation STEMI with static thrombus (Carinal trapping of thrombus ,Coronary Lerish sydrome ) 4. Embolic STEMI with showers of emboli into both LCX and LAD Simultaneous or sequential Anterior and Inferior STEMI 5. Wrap around LAD true Global MI 2. RCA-dependent LAD circulation through collaterals 3.
Cardiogenic shock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset ACS pathophysiology is not that simple.
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? With serial ECGs that are ‘STEMI negative’ the physician could have waited for serial troponin levels or referred the patient as “non-STEMI”. What was the outcome and final diagnosis?
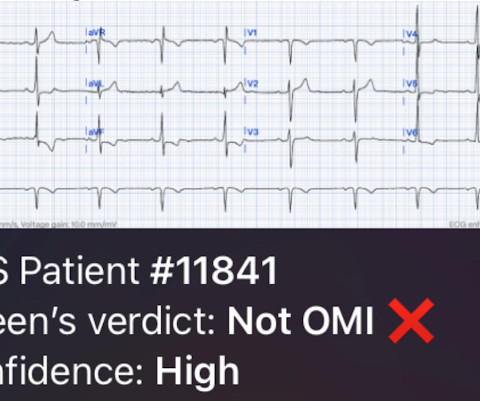
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
STEMI – Anterior Wall ECG shows ST elevation myocardial infarction of anterior wall. Up sloping elevation of ST segment is seen in leads V1 to V5, with maximum ST elevation in V2, as is characteristic of anterior wall infarction.
Implantation of the Impella CP micro-axial flow pump may increase survival at six months among patients with STEMI complicated by cardiogenic shock (CS), according to the results of the DanGer Shock study.
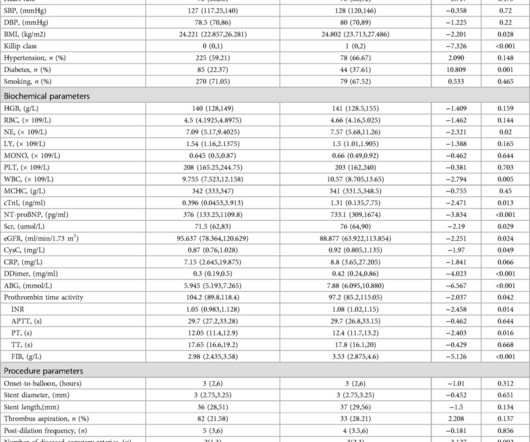
However, whether immediate blood glucose and FIB levels affect coronary blood flow during primary percutaneous coronary intervention (PCI) remains unclear.ObjectiveTo explore the correlation between admission blood glucose (ABG), fibrinogen (FIB) and slow blood flow during primary PCI for acute ST segment elevation myocardial infarction (STEMI).MethodsA
Background Different ST-segment elevation myocardial infarction (STEMI) localizations go along with dissimilarities in the size of the affected myocardium, the causing coronary vessel occlusion, and the right ventricular participation. Results Of the 2,195 patients, 1,118 had an anterior (AWS)- and 1,077 a non-anterior-wall-STEMI (NAWS).
Doing so literally enables those of us who embrace the OMI Paradigm the ability to recognize within seconds that a patient with new CP ( C hest P ain ) — and — one or more hyperacute T waves — needs prompt cath regardless of potential absence of STEMI criteria.
In this ECG Cases blog we look at 10 cases of patients with chest pain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
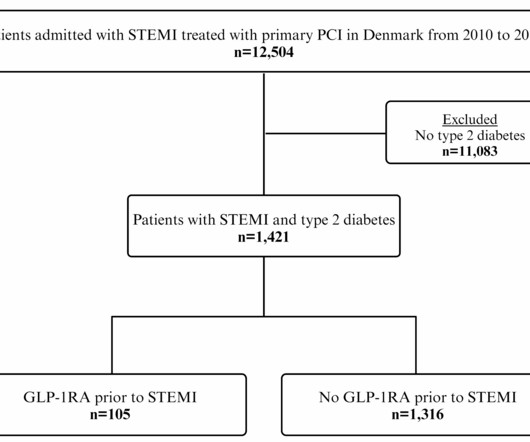
Yet, the impact of GLP-1RA treatment before ST-segment elevation myocardial infarction (STEMI) on. Glucagon-like peptide-1 receptor agonist (GLP-1RA) treatment reduces cardiovascular events in type 2 diabetes.
Primary percutaneous coronary intervention (PPCI) remains the gold-standard treatment for ST-elevation myocardial infarction (STEMI). We present the case of a man in his 50s, admitted with cardiac arrest secondary to inferolateral STEMI.
Implementing and tracking quality improvement (QI) metrics may lead to improved outcomes in patient care after STEMI in low- and middle-income countries (LMIC), according to an analysis of data from the ACC's Global Heart Attack Treatment Initiative (GHATI).
We discover that for STEMI/OMI vs subendocardial ischemia, we should look for STEMI(-)OMI, subacute OMI, and OMI in the presence of LBBB and RBBB, and consider the differential for diffuse ST depression with reciprocal ST elevation in aVR.
A small proportion of patients with STEMI treated via primary PCI experienced late ventricular tachycardia (VT) or ventricular fibrillation (VF), occurring one or more days following the procedure, but late VT or VF with cardiac arrest occurred rarely, especially among patients with uncomplicated STEMI, according to a study published in JAMA Network (..)
7, 2024 — The Society for Cardiovascular Angiography & Interventions (SCAI) recently announced the publication of the Expert Consensus Statement on the Management of Patients with STEMI Referred for Primary PCI. tim.hodson Mon, 10/07/2024 - 14:45 Oct.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content