This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Tricuspid regurgitation (TR) after implantation of cardiovascular implantable electronic devices (CIED) is a concern, possibly due to lead impingement or underlying cardiac abnormalities. While TR after CIED may worsen prognosis,1 data on its progression, riskfactors, and impact on cardiac structure and function are limited.
BackgroundTranscatheter closure of perimembranous ventricular septal defects in children is a highly effective procedure, but it can result in tricuspid regurgitation (TR). TR was evaluated using echocardiography, and multivariate logistic regression was performed to identify independent riskfactors of postprocedural TR.
Tricuspid valve surgery for isolated tricuspid valve disease is becoming increasingly common. Incidence and riskfactors of this complication are not well established. These patients often need permanent pacemaker (PPM) post-surgery.
Abstract Tricuspid regurgitation (TR) is a known complication of cardiac implantable electrical devices (CIEDs), with prevalences ranging from 10% to as high as 30%. A shorter lead-TA-distance was an independent riskfactor for TR deterioration in individuals with post-LBBAP implantation.
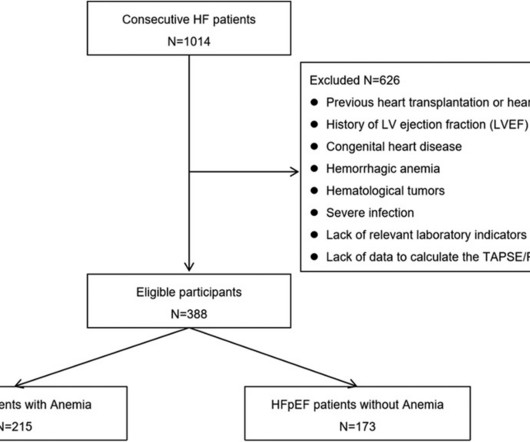
The level of hemoglobin (Hb) had a weak negative linear correlation with NT-pro-BNP (log-transform, r = 0.30, P < 0.0001) and a positively correlation with the tricuspid annular plane systolic excursion (TAPSE)/pulmonary arterial systolic pressure (PASP) ratio (r = 0.44, P < 0.0001).
Herein, we provide an overview of the current knowledge on the pathophysiology and riskfactors for AF in adult congenital heart disease, with a special focus on the existing challenges in AF ablation. Emerging imaging modalities and ablation techniques might have a role to play.
This clinical consensus statement provides a comprehensive overview of low BP in HFrEF, including its definition, riskfactors, and effects of HF therapies on BP. Low blood pressure with major or mild symptoms. **SBP SBP <80mmHg or symptomatic low BP or asymptomatic low BP.
In people aged 75 years, tricuspid and mitral regurgitation were the most prevalent VHD (21.1% Appropriate resources and strategies need to be implemented to minimize racial and ethnic disparities and promote equity in VHD diagnosis and cardiovascular riskfactor management.RegistrationURL:[link] Unique Identifier: NCT05453526.
BackgroundPrior studies investigating the impact of residual mitral regurgitation (MR), tricuspid regurgitation (TR), and elevated predischarge transmitral mean pressure gradient (TMPG) on outcomes after mitral transcatheter edge‐to‐edge repair (TEER) have assessed each parameter in isolation. Overall, mean age was 76.7±10.6
BackgroundData regarding permanent pacemaker (PPM) implantation following tricuspid valve surgery (TVS) are limited. We sought to evaluate its incidence, riskfactors, and outcomes.Methods and ResultsMedicare beneficiaries who underwent TVS from 2013 to 2020 were identified. 1.49],P=0.04). 1.49],P=0.04). 4.75],P<0.0001).
Part 2: Empirical Studies in Cardiac Surgery; Risk Model Recommendations The Annals of Thoracic Surgery January 2022 David Shahian Social RiskFactors in Society of Thoracic Surgeons Risk Models.
Adding LV ejection fraction, tricuspid annular plane systolic excursion (TAPSE) or LA volume index to these models did not alter the association of strain measures of the LV (1.41 (1.06–1.89), p=0.02), RV (1.48 (1.03–2.13), p=0.04) or LA (0.61 (0.49–0.76), p<0.001).
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
However, data focusing specifically on moderate SMR and associated riskfactors are lacking. Background Significant secondary mitral regurgitation (SMR) is known to be associated with worse prognosis. After matching, NYHA class and SMR aetiology remained associated with both outcomes (for both: log rank p<0.050).
MethodsWe prospectively enrolled patients with FD and controls matched for age, sex, and cardiovascular riskfactors. No differences were found for tricuspid annular plane systolic excursion (p=0.073) and RV fractional area change (p=0.461), while RV systolic Tissue Doppler velocity was reduced in patients with FD (p=0.041).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content