This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Objective:A proportion of acute ischemic stroke (AIS) patients suffer from early neurological deterioration (END) within 24 hours following intravenous thrombolysis (IVT), which greatly increases the risk of poor prognosis of these patients.
Patients with elevated traditional riskfactors at admission may benefit more from thrombolytic therapy compared to those with high inflammatory response indicators. Stroke, Volume 56, Issue Suppl_1 , Page ATP20-ATP20, February 1, 2025.
Renal dysfunction, especially chronic kidney disease, is the biggest riskfactor of mortality among thrombolysed stroke patients, according to a retrospective cohort observational study published in Medicine.
Cervical artery dissection occurs as a result of the interplay among riskfactors, minor trauma, anatomic and congenital abnormalities, and genetic predisposition. The diagnosis can be challenging both clinically and radiologically.
Results The two groups were similar in age, riskfactors, comorbidities, and complications. SCAD-STEMI patients more often had Thrombolysis in Myocardial Infarction 3 flow, while type 1 STEMI patients were more often treated with percutaneous coronary intervention and dual antiplatelet therapy.
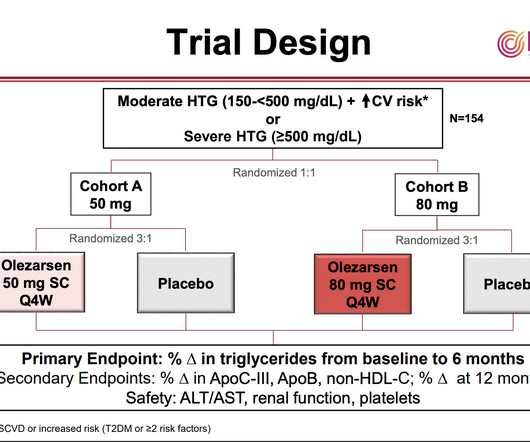
Brian Bergman, MD “Treatments to reduce high triglycerides are an unmet clinical need,” said Brian Bergmark, MD , of the Thrombolysis in Myocardial Infarction (TIMI) Study Group at Brigham and Women’s Hospital and Harvard Medical School and the study’s principal investigator. and Canada. Patients’ median triglyceride level was 242 mg/dL.
BACKGROUND:Established risk models may not be applicable to patients at higher cardiovascular risk with a measured Lp(a) (lipoprotein[a]) level, a causal riskfactor for atherosclerotic cardiovascular disease.METHODS:This was a model development study. Circulation: Genomic and Precision Medicine, Ahead of Print.
Background Microcirculatory dysfunction is an independent riskfactor for a poor prognosis after percutaneous coronary intervention (PCI) in patients with acute myocardial infarction (AMI). Cardiac function was measured by echocardiography during hospitalization and follow-up.
Introduction:Although prior antiplatelet therapy (APT) could potentially contribute to bleeding risk, the influence of prior APT on intravenous thrombolysis outcomes remains controversial. Patients with prior APT were older (72 vs. 66 years), and had a higher prevalence of vascular riskfactors than those without APT.
Background:Despite advances in intravenous thrombolysis and endovascular thrombectomy, numerous acute ischemic stroke survivors continue to experience various disability levels. Subgroup analyses revealed a noteworthy benefit of GTN in the 90-day NIHSS score for non-thrombolysis patients (1 vs 2, p=0.016).
Genetic protein S (PS) deficiency caused by PROS1 gene mutation is an important riskfactor for hereditary thrombophilia.Case introductionIn this case, we report a 28-year-old male patient who developed a severe pulmonary embolism during his visit. The patient had experienced one month of chest pains, coughing and hemoptysis symptoms.
Outcomes included first pass effect (FPE, extended Thrombolysis in Cerebral Infarction [eTICI] 2c/3 after first pass) and favorable outcome (3-month modified Rankin Scale score of 0 to 2 or equal to premorbid mRS score).Results:Of Components of thrombi were quantified using immunostaining.
Hence, we aimed to study the pro-inflammatory and procoagulant responses post-thrombolysis and their contributory role in clinical outcome.Methods:This is a single-center retrospective study of ALT or TNK treated AIS patients admitted to a comprehensive stroke center over a 3-year period. A p-value of <0.05
Background:Diabetes mellitus (DM) is one of the riskfactors for acute ischemic stroke, usually leading to poor prognosis. While DM can reduce the effect of intravenous thrombolysis, metformin can have a positive outcome on AIS patients. Stroke, Volume 55, Issue Suppl_1 , Page AWP5-AWP5, February 1, 2024.
There was no difference between the ALT and TNK cohorts in their baseline demographic characteristics or premorbid vascular riskfactors. Of the 165 patients undergoing thrombolysis, 75 also underwent EVT, with 55 patients treated with ALT compared to 20 patients treated with TNK.
Intravenous thrombolysis is a compelling therapeutic approach, with current limited data suggesting early intervention (4.5 This article provides a narrative review of pathophysiological features, riskfactors, and current and emerging management techniques of CRAO. hours of symptom onset) results in better patient outcomes.
BACKGROUNDIn patients with acute ischemic stroke secondary to large vessel occlusion, achieving modified Thrombolysis in Cerebral Infarction (mTICI) 2c/3 (excellent recanalization) over mTICI 2b is associated with improved functional outcomes. Stroke: Vascular and Interventional Neurology, Ahead of Print.
IntroductionA high level of low‐density lipoprotein ‐ cholesterol (LDL‐C) is a known riskfactor for ischemic stroke1. We collected data on baseline characteristics and demographics, functional outcomes at discharge and 90 days, and procedural information including final thrombolysis in cerebral infarction (TICI) grade.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
Introduction:Because of the risk of infarcted tissue leading to symptomatic intracerebral hemorrhage (sICH) after intravenous thrombolysis for acute ischemic stroke, patients are monitored for at least 24 hours in a critical care setting.
The new analysis of the trial results, led by UVA Health’s Andrew Southerland , MD, found that high blood sugar shortly after thrombolysis – opening blocked arteries in the brain with a clot-busting drug – was associated with greater risk for potentially deadly brain bleeds, particularly in older patients with more severe strokes.
There was no difference in the rate of administration of IV thrombolysis (5.0% Patients with CADASIL, in general, carried a lower burden of vascular riskfactors. They received IV thrombolysis at an equal rate but EVT at a lower rate, likely due to the small vessel pathology of CADASIL. vs 49.8%, p=0.31), obesity (15.0%
Methods In a prospective cohort study, patients with intermediate high-sensitivity cardiac troponin I concentrations (5 ng/L to sex-specific 99th percentile) in whom myocardial infarction was ruled out were enrolled and underwent coronary CT angiography (CCTA) after hospital discharge.
Some of the latest strategies include: Innovations in Thrombolysis and Clot Retrieval : Techniques such as tissue plasminogen activator (tPA) injections and mechanical thrombectomy are significantly improving recovery rates for ischemic stroke patients.
We fit logistic regression models adjusted for age, race/ethnicity, Charlson index, household income by ZIP code, administration of IV thrombolysis or thrombectomy (EVT), hospital teaching status, census region, and bedsize.Results:We included 434,463 IS discharges, of which 1,407 had APLS.
Other riskfactors remained unchanged. Intravenous thrombolysis and mechanical thrombectomy rates increased over time from 2008 to 2010 to 2017 to 2019 (9.5%–13.8% Secular trends for patient characteristics, treatments, and outcomes were analyzed.RESULTS:A total of 7050 eligible patients (mean age, 43.1; years (Ptrend=0.01).
Meschia is a pioneer in the study of inherited riskfactors for ischemic stroke and has had a longstanding commitment to providing the latest evidence for carotid revascularization as a means for stroke prevention. Meschia is certified by the American Board of Psychiatry and Neurology (ABPN) in neurology and vascular neurology.
Why systemic hypertension is a weak coronary riskfactor ? Unlike the brain, where stroke risk is directly related to systolic BP, fortunately sudden systolic spikes never get a chance to attack the coronary endothelium as much of the coronary lumen is closed during most periods of systole. of course at the cost of failure).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content