This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
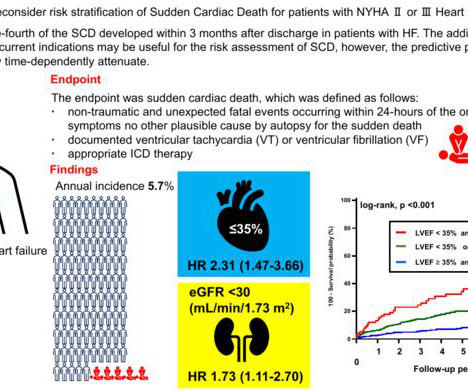
Background High-intensity physical activity has traditionally been discouraged in patients with hypertrophic cardiomyopathy due to concerns about triggering suddencardiacdeath. However, current guidelines adopt a more liberal stance, and evidence on riskfactors for exercise-related suddencardiacdeath remains limited.
Image courtesy of Yoshihiro Sobue from Fujita Health University mtaschetta-millane Tue, 07/30/2024 - 09:18 July 30, 2024 — Patients with congestive heart failure (CHF) having a compromised blood supply, are at greater risk of suddencardiacdeath (SCD).
SCAD can cause acute coronary syndrome and myocardial infarction (MI), as well as suddencardiacdeath. It presents similarly to atherosclerotic MI although typically in patients with few or no atherosclerotic riskfactors, and particularly in women.
Suddencardiacdeath is an important cause of mortality in patients with kidney failure undergoing renal replacement therapy, either hemodialysis or peritoneal dialysis. The riskfactors associated with suddencardiacdeath in these patients only partly overlap with those in the general population.
Identifying children with hypertrophic cardiomyopathy (HCM) at high risk for suddencardiacdeath (SCD) is an important part of clinical care.1,2 Identifying children with hypertrophic cardiomyopathy (HCM) at high risk for suddencardiacdeath (SCD) is an important part of clinical care.1,2
Possible arrhythmic recurrences and the risk of suddencardiacdeath (SCD) in this setting are reasons for concern, and limited data have been published to guide clinical management of these patients. Gender and anteroseptal late gadolinium enhancement were not found as potential riskfactors in this analysis.
Abstract The limited literature and increasing interest in studies on cardiac electrophysiology, explicitly focusing on cardiac ion channelopathies and suddencardiacdeath in diverse populations, has prompted a comprehensive examination of existing research.
Suddencardiacdeath (SCD) risk stratification is based on clinically recognized riskfactors (RF), such as reduced left ventricular (LV) ejection fraction (EF), heart failure (HF), prior myocardial infarction (MI), and syncope. These RFs fail to capture the majority of SCDs.
Unlike a heart attack, cardiac arrest is an electrical malfunction that causes the heart to stop beating suddenly. Without immediate intervention, suddencardiacdeath can occur within minutes. This results in a failure to pump blood to the brain and other vital organs.
Background:Limited data exist on the incidence of severe QT prolongation (SQTP) in patients using antipsychotics or antidepressants and the associated risk of ventricular arrhythmias (VA) and suddencardiacdeath (SCD).Aims:This ms and +6.7 ± 36.1 ms, respectively.
There is an unmet need for better risk stratification for suddencardiacdeath in the era of primary prevention ICD therapy. Scar burden on LGE-CMR imaging may be a risk marker for ventricular arrhythmia post-myocardial infarction (MI).
Hypertrophic cardiomyopathy (HCM) stands as one of the most common inheritable myocardial disease and is often marked by its association with suddencardiacdeath (SCD) in the young. 1 2 Traditionally, risk assessment in HCM has focused mainly on estimating the likelihood of SCD.
Publication date: Available online 18 April 2024 Source: The American Journal of Cardiology Author(s): Xinyu Zhu, Yuan Tian, Ying Shi, Jianxiu Lian, Honghu Shen, Lulu Li, Haishan Wu, Pengfei Liu
Suddencardiacdeath (SCD) is one of the most important causes of mortality in the world. Myocardial infarction (MI) is a major riskfactor for SCD associated with significant pro-arrhythmic structural and electrophysiological ventricular remodelling.
BackgroundSpontaneous coronary artery dissection (SCAD) is an increasingly recognized cause of acute coronary syndrome or suddencardiacdeath, primarily affecting relatively young women (median age, 51 years) without typical cardiovascular riskfactors.
However, the cause and riskfactors for mortality remain uncertain.MethodsThis retrospective, singlecenter study identified children with primary and secondary pulmonary vein stenosis through a cardiac catheterization database. Journal of the American Heart Association, Ahead of Print. 95% CI, 2.214.1];P<0.001).
The multicenter randomized trial, known as AGENT IDE , enrolled participants with in-stent restenosis, all of whom had high rates of coronary riskfactors; more than half had diabetes and nearly 80 percent previously had two or more major coronary arteries partially or completely blocked.
Low and borderline ABIs were associated with an increased risk of SCD (demographically adjusted hazard ratios [HRs], 2.27 [95% CI, 1.64–3.14] The association between low ABI and SCD remained significant after adjustment for traditional cardiovascular riskfactors (HR, 1.63 [95% CI, 1.15–2.32]).ConclusionsLow
However, a subset of patients may develop arrhythmic complications, including suddencardiac arrest and suddencardiacdeath. We propose an algorithm integrating clinical, rhythmic, echocardiographic, CMR, and Positron Emission Tomography/CMR parameters for arrhythmic risk stratification and management.
Sudden arrhythmic death syndrome (SADS), characterized by an unknown or inconclusive cause of death at autopsy, together with a negative or non-lethal toxicology screening, is the most common cause of suddencardiacdeath (SCD) in victims under the age of 35.
ABSTRACT Arrhythmogenic cardiomyopathy (ACM) is a genetically heterogeneous inherited cardiomyopathy with an estimated prevalence of 1:500010000 that predisposes patients to life-threatening ventricular arrhythmias (VA) and suddencardiacdeath (SCD).
Abstract Introduction Most patients with Brugada syndrome (BrS) are first diagnosed in their 40s, with suddencardiacdeath (SCD) often occurring in their 50s. This study aimed to assess the incidence and riskfactors for late life-threatening arrhythmias in patients with BrS.
On competing risk regression analysis, absolute LV-GLS ≤ 9% was associated with a higher rate of primary endpoints (subhazard ratio: 2.66 [95% confidence interval: 1.96 to 3.36]) after adjustment for known riskfactors. 003) and 2022 ESC risk model (log-likelihood ratios, -268.4 vs -266.2; vs -264.9;
We can also use intracardiac echocardiography to guide and facilitate the procedure with real-time visualisation of the cardiac structures being treated.” 50 year trends in atrial fibrillation prevalence, incidence, riskfactors, and mortality in the Framingham Heart Study: a cohort study. 2018;20(1):e1-e160. Eur Heart J.
The Smidt Heart Institute recently received CAROL Act funding to study the connection between ventricular arrhythmias—abnormal heartbeats that start in the heart’s two lower chambers—and an elevated risk of suddencardiacdeath in patients with mitral valve disease.
11 Despite the link between inflammation and cardiovascular disease has been proven by extensive research, most physicians have focused on treating high-risk patients with lipid lowering therapies including statin therapy.1,12,13 For most patients we can use high sensitivity C-reactive protein (hsCRP) to determine residual inflammatory risk.21-23
Riskfactors of suddencardiacdeath in hypertrophic cardiomyopathy. A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Journal of the American College of Cardiology and Circulation, 58, e212-260. Hong Y, Su WW, Li X.
This discussion comes from this previous post: Hyperthermia and ST Elevation Discussion Brugada Type 1 ECG changes are associated with suddencardiacdeath (SCD) and the occurrence of ventricular dysrhythmias. Patients that develop a Type 1 pattern without any precipitating or provoking factors have a risk of SCD of 0.5-0.8%
What caused these 729 deaths (filtered out of 29000 deaths) I understand physical autopsy could not be done in majority of deaths (Even in witnessed , in hospital deaths). Is it suddencardiacdeath ? Is it sudden “non cardiac ” death ? So, the question remains.
No family history of suddencardiacdeath, cardiomyopathy, premature CAD, or other cardiac issues. Smith Major Learning Point: The worst riskfactor for a bad outcome in OMI is young age because cardiologists cannot believe that a young person can have an OMI. No similar symptoms in the past.
Furthermore, it includes the latest recommendations which specifically address AF and thromboembolic risk assessment, anticoagulation, left atrial appendage occlusion, AF catheter or surgical ablation, and riskfactor modification and AF prevention. million.
Background and Formulas : QT interval prolongation is widely used as an important riskfactor for progression to torsades de pointes (TdP) and possible subsequent death. Correlation of QT Interval Correction Methods During Atrial Fibrillation and Sinus Rhythm. Am J Cardiol 12(9):1379-1383; Nov 2013.
Suddencardiacdeath in cardiomyoptahies: incidence, riskfactors and prevention. Significant LGE at CMR; LVEF <50%; abnormal blood pressure response during exercise test; LV apical aneurysm; high-risk genotype. It occurs at a rate ranging between 0.15% and 0.7%
Recent research has shown that cardiovascular disease is higher in persons living with HIV compared with individuals without HIV, with an estimated 4-fold higher rate of suddencardiacdeath compared with the general population. million lives so far.
Fever not only unmasks a Brugada-type electrocardiogram (ECG) but also increases the risk of ventricular tachyarrhythmias such as ventricular fibrillation (VF) or suddencardiacdeath. Conclusion of this paper: Fever is a great riskfactor for arrhythmia events in Brugada Syndrome patients. months).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content