This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
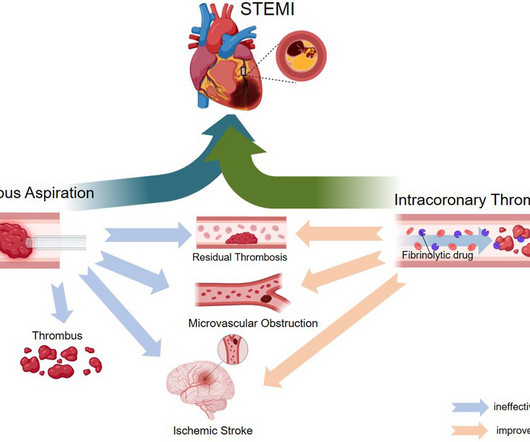
ST-elevation myocardial infarction (STEMI) is a critical cardiovascular emergency characterized by acute coronary artery occlusion and subsequent myocardial injury. The pathophysiology of MVO is systematically reviewed, followed by an evaluation of clinical studies on thrombus aspiration and intracoronary thrombolysis in STEMI management.
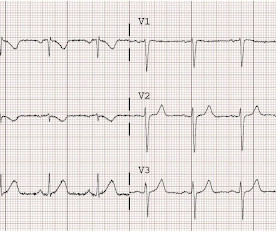
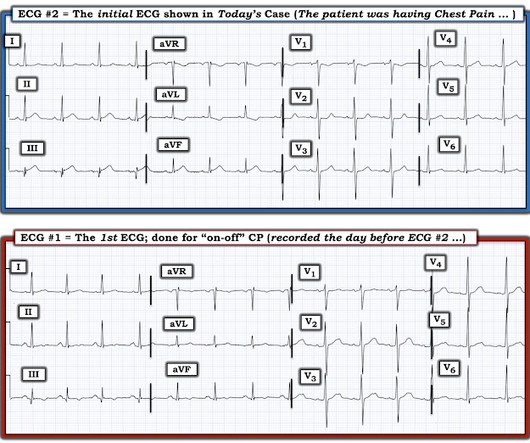
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
Doing so literally enables those of us who embrace the OMI Paradigm the ability to recognize within seconds that a patient with new CP ( C hest P ain ) — and — one or more hyperacute T waves — needs prompt cath regardless of potential absence of STEMI criteria.
STEMI remains a major cause of morbidity, mortality, disability, and high health care costs in Latin America and the rest of the world. New data assessing the impact of ACC's Global Heart Attack Initiative (GHATI) on patient care outcomes at the CEDIMAT Cardiovascular Center in Santo Domingo, Dominican Republic.
Cardiogenic shock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset ACS pathophysiology is not that simple.
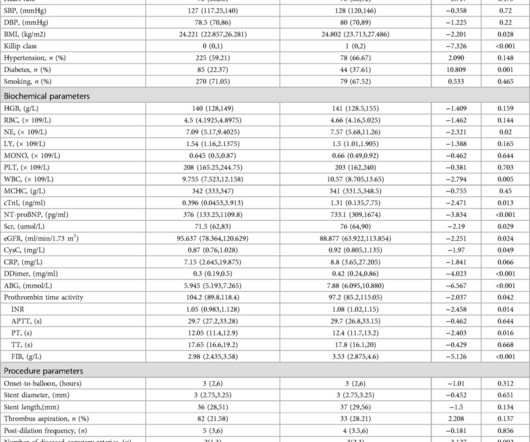
However, whether immediate blood glucose and FIB levels affect coronary blood flow during primary percutaneous coronary intervention (PCI) remains unclear.ObjectiveTo explore the correlation between admission blood glucose (ABG), fibrinogen (FIB) and slow blood flow during primary PCI for acute ST segment elevation myocardial infarction (STEMI).MethodsA
The Minneapolis Heart Institute Foundation (MHIF) is presenting leading research focused on trends in ST-elevation myocardial infarction (STEMI), the most severe form of a heart attack, at the American College of Cardiology’s Annual Scientific Session (ACC.24), 24), being held April 6-8 in Atltanta, GA.
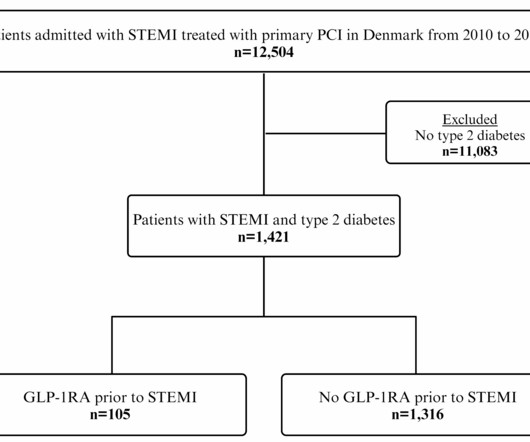
Yet, the impact of GLP-1RA treatment before ST-segment elevation myocardial infarction (STEMI) on. Glucagon-like peptide-1 receptor agonist (GLP-1RA) treatment reduces cardiovascular events in type 2 diabetes.
7, 2024 — The Society for Cardiovascular Angiography & Interventions (SCAI) recently announced the publication of the Expert Consensus Statement on the Management of Patients with STEMI Referred for Primary PCI. tim.hodson Mon, 10/07/2024 - 14:45 Oct.
[link] == MY Comment, by K EN G RAUER, MD ( 8/6 /2023 ): == Brilliant talk by Dr. Smith on the state of the art addressing the “need for OMI — and the fallacy of STEMI”. The current STEMI paradigm that continues to be followed by all-too-many clinicians ( including all-too-many cardiologists ) is fallacious.
This investigator-initiated study was conducted by the University of Calgary, was funded by the Canadian Institute of Health Research, and enrolled patients across 22 stroke centers in Canada. TNKase is also FDA-approved for the treatment of acute ST-elevation myocardial infarction (STEMI) in adults. For more information, go to [link].
Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.) The cath lab was activated prehospital But imagine if the patient had walked in.
” R outine nasal Oxygen has little use in the management of STEMI. Now,14 years later, some young researchers reaching out to this concept ,via liquid myocardial oxygen. It is tough to consider oxygen as a “powerful and magical drug”, because it is freely available everywhere.”
He called 911 and paramedics recorded a prehospital 12 lead ECG which showed a clear inferior STEMI (not shown, tracing could not be found). To diagnose inferior MI, there must always be reciprocal ST depression or T-wave inversion or both in lead aVL (see abstract of our research below). Research presented at 2011 SAEM in Boston.
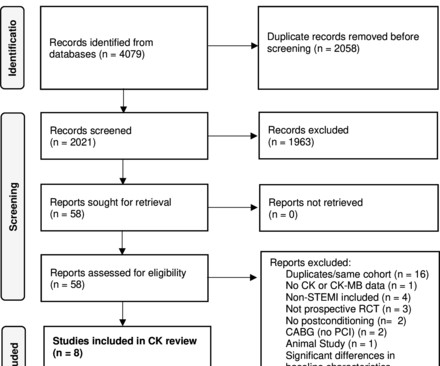
Objectives This study aimed to perform a meta-analysis of the short-term impact of ischaemic postconditioning (IPoC) on myocardial injury in ST elevation myocardial infarction (STEMI) using surrogate cardiac biomarkers. Conclusions IPoC does not seem to protect against myocardial injury in STEMI, except possibly in smokers.
Contemporary research studies of MINOCA have evaluated the prognosis of these patients, reporting a 12-month all-cause mortality of 4.7% (95% confidence interval, 2.6–6.9), This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. Circulation. 2017;135(16):1490–3. Available from: [link] 4.
Percutaneous coronary intervention (PCI) can effectively restore myocardial perfusion in patients with ST-segment elevation myocardial infarction (STEMI). Nevertheless, STEMI patients may still experience a n.
BackgroundCurrent research suggests that microvascular obstruction (MVO) following the first percutaneous coronary intervention (PCI) in myocardial infarction patients is closely related to inflammatory responses. The predictive model incorporating LCR enhances the ability to predict MVO occurrence in patients with STEMI post-PCI.
Although there are more criteria to consider when looking for OMIs compared to STEMIs, anyone can learn them, and this guide is intended to help accelerate that process! On each device — the large-print labels on the guide instantly take you to concise summary of research-based ECG criteria developed by Drs.
Background Despite restoration of epicardial blood flow in acute ST-elevation myocardial infarction (STEMI), inadequate microcirculatory perfusion is common and portends a poor prognosis. Further research is needed to optimise the selection of thrombolytic agents and treatment protocols. to 2.40; I 2 =0%; p=0.12).
BackgroundThe pharmacoinvasive (PhI) strategy is the standard-of-care for ST-elevation myocardial infarction (STEMI) patients when primary percutaneous coronary intervention (pPCI) is unfeasible. Further research should develop evidence-based lysis-PCI protocols that optimize both clinical outcomes and cost-effectiveness.
Methods A retrospective clinical cohort study was performed using data from the English National Institute for Health Research Health Informatics Collaborative (2010–2017). to 0.64) after non-ST-elevation (NSTE)-ACS and one-third as likely after STEMI (OR 0.30, 95% CI 0.19 After STEMI, the respective ORs were 1.20 (95% CI 0.84
The benefits of complete revascularization over culprit-only coronary artery revascularization were confirmed in older patients with ST-segment elevation myocardial infarction (STEMI) and multivessel disease over the first 4 years, according to late-breaking research presented in a Hot Line session today at ESC Congress 2024.
IntroductionHypoxic liver injury (HLI) and Killip classification are poor prognostic factors in patients with ST-segment elevation myocardial infarction (STEMI). Early recognition of HLI and accurate assessment of Killip classification is warranted for effective management of STEMI.
In cardiovascular research, serotonin has been implicated in modulating vascular tone, platelet aggregation, and myocardial function. Conclusion:Higher 5-HTP levels are independently associated with a reduced risk of MACE in patients after STEMI. Circulation, Volume 150, Issue Suppl_1 , Page A4141170-A4141170, November 12, 2024.
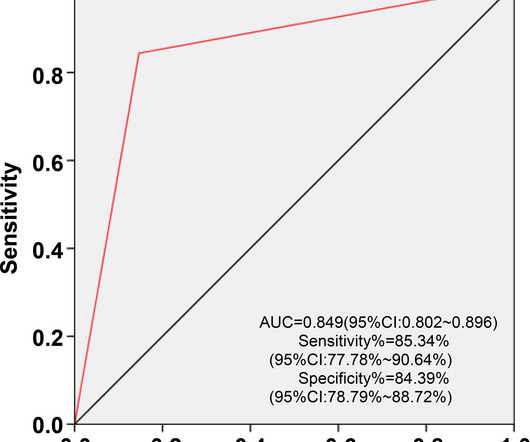
However, its prognostic role following percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardial infarction (STEMI) remains unclear. And the NHR was analyzed using receiver operating characteristic (ROC) curves to predict the occurrence of postoperative LVR and MACE in STEMI patients.
Moreover, the research which appears to confirm this idea was indeed in relation to the circumflex, but they did not study Occlusion ; rather, they studied asymptomatic coronary disease. I am glad that Ken Grauer (below) brings up the issue of whether the presence of "T-wave in V1 taller than T-wave in V6" is evidence for OMI.
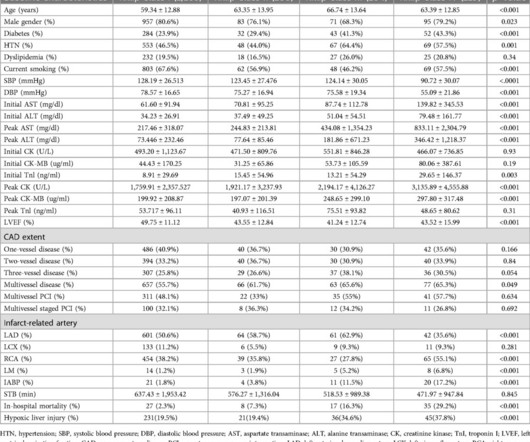
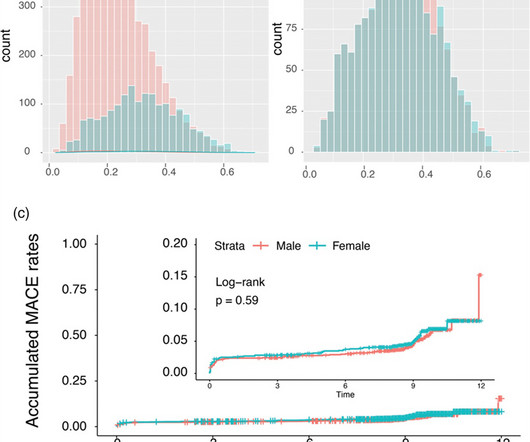
Background: Gender-specific outcomes after percutaneous coronary interventions were studied by a number of research groups with different endpoints and cohorts of different ethnic extractions. In the unmatched STEMI subgroup, all-cause mortality was significantly higher in females driven by older age (P < 0.001). vs. 5.2%; P = 0.749).
Data sources Linked Clinical Practice Research Datalink (CPRD) and Hospital Episode Statistics (HES). Interventions Aspirin and clopidogrel (AC, reference) versus aspirin and prasugrel (AP) or aspirin and ticagrelor (AT); AP evaluated only in patients with ST-elevation myocardial infarction (STEMI). Setting Primary and secondary care.
Furthermore, some ECGs may not meet the STEMI criteria but may still be diagnostic for acute coronary occlusion (ACO). Many researchers, including the editors of this blog, tried to develop such tools in the recent past and we have recommended their use in certain clinical scenarios in many posts on this blog.
Background Despite improvements in outcomes of ST elevation myocardial infarction (STEMI), ventricular septal rupture (VSR) remains a known complication, carrying high mortality. The contemporary incidence, mortality, and management of post-STEMI VSR remains unclear. In-hospital mortality was 73.6 ± 1.8%, but only 29.2 ± 1.9
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? Circulation Research , 56 (2), 184–194. About one hour later his high sensitivity troponin I resulted at 3,000 ng/L (reference 3-54 ng/L). The patient continued having chest pain. What is the rhythm?
Purpose Construction of a prediction model to predict the risk of major adverse cardiovascular events (MACE) in the long term after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardial infarction (STEMI).
Aim Acute injury and subsequent remodelling responses to ST-segment elevation myocardial infarction (STEMI) are major determinants of clinical outcome. Methods and results miRs were quantified in blood samples obtained from patients after primary PCI (PPCI) for STEMI.
Analyses of STEMI and Neither the primary or secondary endpoints of NSTEMI patients were significantly different.ConclusionsIn this post-hoc analysis of the FRAME-AMI trial, no significant difference in clinical outcomes was observed between the immediate and staged CR strategies for AMI with MVD and the subgroups, such as STEMI or NSTEMI.
Now let’s compare this with the existing paradigm to identify multiple preventable delays to reperfusion, which can be improved through the paradigm shift from STEMI to OMI. Therefore, cardiologists in general should not be used as the reference standard for interpreting OMI on the ECG, either in clinical practice or in research papers.
Barely any STE, and thus not meeting STEMI criteria. Annals of Emergency Medicine Cardiology was called to evaluate the patient immediately for emergent cath, but they stated that the ECG did not meet STEMI criteria and elected to wait for further information before proceeding with cath. He was given 6mg IV morphine for ongoing pain.
Background Despite advances in percutaneous coronary intervention (PCI) for ST segment elevation myocardial infarction (STEMI), in-hospital mortality remains a concern, highlighting the need for the identification of additional risk factors such as serum iron levels. μmol/L) and a control group (Fe ≥7.8 μmol/L).
Stress hyperglycemia ratio (SHR), associated with adverse outcomes in patients with ST-segment elevation myocardial infarction (STEMI), has several definitions. This study aims to assess the prognostic value o.
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Evidence for Wellens as a reperfusion syndrome To my knowledge, there is no research paper demonstrating this. Is it normal STE?
The primary safety end point was Bleeding Academic Research Consortium 3 to 5 bleeding at 30 days.RESULTS:Between January 10, 2019, and September 18, 2021, a total of 2989 patients were randomized. The primary efficacy end point occurred in 37 patients (2.5%) in both the PPA and placebo groups (hazard ratio, 1.00 [95% CI, 0.63
“ Since Intravenous lysis looks too simplistic, that do not need expertise, and lacks a commercial trail, it is wrongly depicted as inferior management strategy in STEMI “ Every one of us is equally responsible for this sorry state of affairs. In LAD STEMI time is more crucial. NRMI data Ref 2) 2.There
Methods This prospective study included 258 patients who presented at our center with STEMI, and underwent coronary angiography (CAG). The triglyceride/HDL-C ratio was calculated, and the relationship of this ratio with the SYNTAX score was determined with univariate and multivariate linear regression analyses.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content