This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Stavros Zanos is the senior author on the new bioelectronic medicine ultrasound paper. Credit: Feinstein Institutes) milla1cf Wed, 05/08/2024 - 10:57 May 8, 2024 — Ultrasound could one day complement or even replace drugs to treat diseases.
BACKGROUND:Prior clinical trials have demonstrated the efficacy of ultrasound-facilitated catheter-directed thrombolysis (USCDT) for the treatment of acute intermediate-risk pulmonary embolism (PE) using reduced thrombolytic doses and shorter infusion durations. Circulation: Cardiovascular Interventions, Ahead of Print.
They looked at anonymous results for 57,531 adult patients who underwent pulmonary resection—removal of all or part of a lung—between January 2009 and June 2021. occurrence of postoperative PE in patients undergoing a first-time pulmonary resection for lung cancer. occurrence of postoperative VTE and a 1.3%
The incorporation of artificial intelligence (AI) into point-of-care ultrasound (POCUS) platforms has rapidly increased. The number of B-lines present on lung ultrasound (LUS) serve as a useful tool for the as.
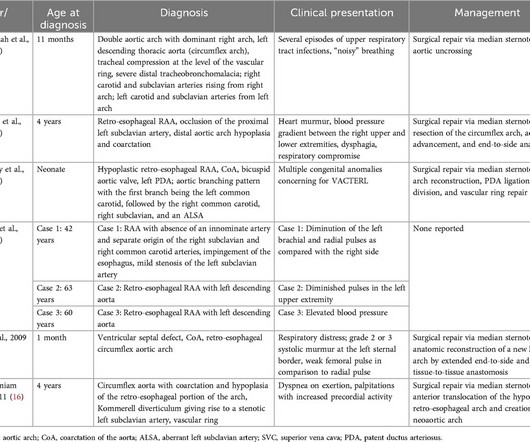
In the setting of circumflex right aortic arch with the ductus arteriosus connecting the left descending aorta and left pulmonary artery, a vascular ring is present and can cause compressive symptoms of the aerodigestive tract.
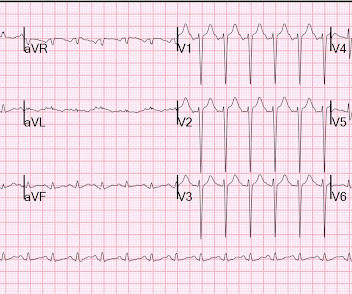
He was started on a heparin drip and CTA of the chest was ordered to rule out pulmonary embolism. This is a case like many others posted (see list below) and the EKG from the patient’s original presentation can be quickly recognized as diagnostic for pulmonary embolism. Now another, with ultrasound. In fact, Kosuge et al.
In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonary embolism. Answer : Bedside ultrasound! Smith : RV infarct may also have this appearance on ultrasound. In PE, there is almost always some hypoxia without any pulmonary edema. So CT is required to find the diagnosis!
Notably, acute massive pulmonary embolism (PE) with bilateral atrial thrombosis is an exceptional occurrence in CAPS. Acute pulmonary embolism (PE) is a common cardiovascular disease that progresses rapidly and has a high mortality rate. It primarily affects small vessels, seldom impacting large vessels.
This Best Case Ever elucidates the practical challenges of working up pregnant patients in the ED with a suspicion of pulmonary embolism. Since this recording, the first ever multi-center prospective outcome study looking at the pulmonary embolism workup in pregnancy was published in the Annals of Internal Medicine.
n=42; median RAP, 4 mm Hg; pulmonary capillary wedge pressure, 11 mm Hg), those with a low JV distensibility ratio (≤1.6; BACKGROUND:Clinical evaluation of central venous pressure is difficult, depends on experience, and is often inaccurate in patients with chronic advanced heart failure. versus 18.2%; log-rankP=0.034).CONCLUSIONS:Ultrasound-assessed
He was requiring supplemental oxygen and an initial bedside cardiac ultrasound was unremarkable. Despite his large clot burden, there was absence of obstructive shock.Transthoracic Echocardiogram and bilateral duplex venous ultrasound were obtained to evaluate for right heart strain and clot burden. Cardiology was consulted.
Genetic protein S (PS) deficiency caused by PROS1 gene mutation is an important risk factor for hereditary thrombophilia.Case introductionIn this case, we report a 28-year-old male patient who developed a severe pulmonary embolism during his visit. Ultrasound showed no thrombosis in the veins of both lower limbs.
He was in acute distress from pulmonary edema, with a BP of 180/110, pulse 110. He had diffuse crackles on exam and B-lines on chest ultrasound, and chest x-ray also confirmed pulmonary edema. The hypertension alone is the likely etiology of the pulmonary edema. He had no chest pain. The cath lab was activated.
A venous Doppler ultrasound revealed an extensive right lower extremity DVT. Further imaging with a computed tomography (CT) pulmonary embolism (PE) protocol scan of the chest and abdomen identified IVC agenesis along with pulmonary emboli in the left central pulmonary arteries.
We have seen this pattern in many pts with acute right heart strain on this blog. __ Smith : The combination of T-wave inversion in V1-V3 and in lead III is very specific for acute pulmonary embolism. Acute pulmonary embolism was confirmed on CT: The patient did well with treatment. Now another, with ultrasound. This is a quiz.
She had acute pulmonary edema on exam. On arrival, lung ultrasound confirmed pulmonary edema (B lines). A 49 year old woman with h/o COPD only presented with sudden dyspnea. There is STE and hyperacute T-waves in V2 and V3, with significant STE in I and aVL, and inferior reciprocal STD.
A pulmonaryultrasound was performed on admission and was considered positive (PE+) when there were three or more B-lines in two quadrants or more of each hemithorax. Conclusion Lung ultrasound and a high NT-proBNP (3647 ng/L in our series) on admission are the best predictors of acute heart failure needing MV in the first 48 h of ACS.
Abstract Aims A cardiovascular magnetic resonance (CMR) approach to non-invasively estimate left ventricular (LV) filling pressure was recently developed and shown to correlate with invasively measured pulmonary capillary wedge pressure (PCWP). Mean CMR-PCWP decreased from baseline to 36weeks by 0.37 (95% confidence interval 0.78
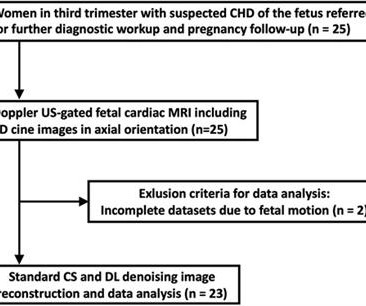
Purpose This study aims to evaluate deep learning (DL) denoising reconstructions for image quality improvement of Doppler ultrasound (DUS)-gated fetal cardiac MRI in congenital heart disease (CHD). Cine imaging was acquired using a balanced steady-state free precession (bSSFP) sequence with Doppler ultrasound gating. vs. 8.3 ± 3.6,
Background Postoperative pulmonary complications (PPCs) after one-lung ventilation (OLV) significantly impact patient prognosis and quality of life. The lung ultrasound score (LUS) was assessed following anesthesia and resuscitation (T5). The occurrence of atelectasis was documented immediately after the surgery.
Additionally, we had to go to a high risk OBGYN for an additional ultrasound to make sure Austin’s heart chambers developed properly (everything appeared OK at the time). It would be a lie to say that Austin didn’t have odds against him. During pregnancy, we learned I had velamentous cord insertion, requiring close monitoring.
This case was posted on the [link] ultrasound site, of which this ECG blog is a part. I refer you to the video case presentation by one of my colleagues, Dr. Rob Reardon (who has, by the way, a fantastic collection of ED ultrasound cases). However, only the first ECG was shown, and it was recorded before the patient became ill.
Bedside cardiac ultrasound showed moderately decreased LV function. CT of the chest showed no pulmonary embolism but bibasilar infiltrates. (And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status.
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Bedside ultrasound showed volume depletion and no pulmonary edema. SVT with aberrancy?
Publication date: Available online 15 December 2023 Source: The American Journal of Cardiology Author(s): Alberto Palazzuoli, Alessandra Cartocci, Filippo Pirrotta, Maria Cristina Tavera, Francesco Morrone, Francesca Vannuccini, Alessandro Campora, Gaetano Ruocco
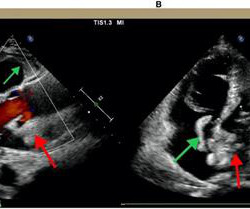
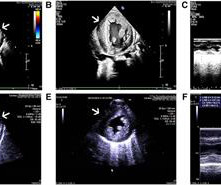
A bedside cardiac ultrasound was recorded: Here is a still image of the echo: The red arrows outline the right ventricle and the yellow arrows outline the left ventricle chamber. It makes pulmonary embolism (PE) very likely. The small LV implies very low LV filling pressures, which implies low pulmonary venous pressure.
This comprehensive evaluation included the use of ultrasound echocardiograms, computed tomography (CT) scans, electrocardiograms, mutagenesis analysis, and structural analysis to gain insights into the patient's condition and the underlying mechanisms of PD. Further genetic testing identified a homozygous mutation c.2662G>T
Ken (below) is appropriately worried about pulmonary embolism from the ECG. What I had not told him before he made that judgement is that the patient also had ultrasound B-lines of pulmonary edema. I was told that the Queen of Hearts had called it OMI with high confidence. What do you think?
Some of the other useful parameters are mitral E velocity deceleration time, changes in mitral inflow with Valsalva maneuver, mitral L velocity, isovolumic relaxation time, left atrial maximum volume index, pulmonary vein systolic/diastolic velocity ratio, color M-mode Vp and E/Vp ratio. J Cardiovasc Ultrasound. Ha J et al.
The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonary embolism). CT angiogram showed extensive saddle pulmonary embolism. Now another, with ultrasound. On epinephrine and norepinephrine drips."
Rob always wished he had x-ray vision…but since he possesses no special powers…using Point-of-Care Ultrasound (POCUS) is the next closest thing. Robert Simard, an Emergency Physician at North York General Hospital and Sunnybrook Health Sciences Centre in Toronto.
Smith comment: before reading anything else, this case screamed pulmonary embolism to me. I would do bedside ultrasound to look at the RV, look for B lines as a cause of hypoxia (which would support OMI, and argue against PE), and if any doubt persists, a rapid CT pulmonary angiogram.
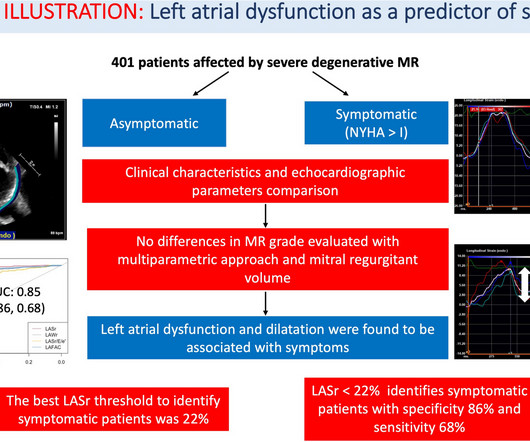
Left atrium (LA) is far from simply being a passive connection chamber between left ventricle and the pulmonary circulation. In patients affected by mitral regurgitation (MR) an impairment in LA compliance and.
Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. The estimated pulmonary artery systolic pressure is 23 mmHg + RA pressure. He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. Here is the initial ED ECG. What do you think?
Right ventricular myocardial work (RVMW) assessed by transthoracic echocardiography allows to study the right ventricular (RV) function using RV pressure-strain loops. The assessment of these novel indexes of.
The following scan revealed a rare vascular ring, which was identified as BDA extending from the confluent of the left pulmonary artery and right pulmonary artery, completely encircling the trachea to form an “O”-shaped vascular ring before finally converging into the descending aorta.
My opinion was that it was not a cath lab case, but I did suggest they do a bedside ultrasound to look for an anterior wall motion abnormality. The RV was small and IVC empty, making pulmonary embolism extremely unlikely. The RV was small and IVC empty, making pulmonary embolism extremely unlikely.
Case Continued Bedside ultrasound was performed: This shows an anterior wall motion abnormality, and highly suggests the LAD as the infarct artery. The patient was slightly tachypneic and mildly hypoxic in the stabilization room and therefore the physicians obtained a CT pulmonary angiogram as well as aortogram to rule out dissection and PE.
In this month's EM Quick Hits podcast, Anand Swaminathan on tips and tricks in polytrauma, Rohit Mohindra on diagnosis and management of toxic megacolon, Jesse McLaren on ECG in pulmonary embolism, Victoria Myers on approach to the patch call for cardiac arrest, Brit Long on when to do a CT head before LP, Salim Rezaie on nebulized ketamine - the ketaBAN (..)
The updated workflow indicates that direct imaging guidance, such as ultrasound, may be used as an alternative to fluoroscopy. "As This is the most commonly used ablation catheter in the world for RF ablation and is fully integrated with the CARTO 3 System. 1 These included one pseudoaneurysm, one PV stenosis and one hematoma.1
In SCAPE (sympathetic crashing acute pulmonary edema), Emergency providers seem now to regularly give high dose NTG, but when the BP is 170/105 in a patient who is not crashing, we often fail to give something to lower afterload. __ Here are some Images: The red circle shows the LAD coursing down the anterior interventricular sulcus.
Abstract Introduction Esophageal injury is one of the most serious complications of pulmonary vein isolation (PVI) with thermic energy sources. Better tissue selectivity of primarily non-thermic pulsed field ablation (PFA) may eliminate collateral injury, particularly the risk of atrio-esophageal fistula (AEF).
To me, this looks like pulmonary edema. A bedside ultrasound was done, with dozens of clips, and was even done with Speckle Tracking. B-line predominance bilateral lungs indicates pulmonary edema. B-line predominance bilateral lungs indicates pulmonary edema. The patient did not have a cough or fever.
Rupture can be either free wall rupture (causing tamonade) or septal rupture, causing ventricular septal defect with left to right flow and resulting pulmonary edema and shock. If detected early by ultrasound, the patient can be saved. 3) Oliva et al. (3)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content