This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In tricuspid valve regurgitation, a complex condition that Cedars-Sinai experts regularly treat, the valve between two heart chambers on the right side doesn't open or close properly. Makkar explained the advances for patients with tricuspid valve disease in a conversationwith the Cedars-Sinai Newsroom. Image by Getty. Image by Getty.
The tricuspid valve (TV), historically deemed the ’forgotten valve’, is undergoing a renaissance as mounting evidence highlights its critical role in cardiovascular outcomes. Severe TR has been independently associated with increased mortality, regardless of left ventricular (LV) function or pulmonary pressures.
Tricuspid valve disease is an often underrecognized clinical problem that is associated with significant morbidity and mortality. Unfortunately, patients will often present late in their disease course with severe right-sided heart failure, pulmonary hypertension, and life-limiting symptoms that have few durable treatment options.
Transcipt of video: Mild tricuspid regurgitation is often noted on echocadiogram reports and sometimes causes a little bit of worry and a lot of questions are asked on mild tricuspid regurgitation. What is this mild tricuspid regurgitation? And mild tricuspid regurgitation is just a small leak from the tricuspid valve.
Tetralogy of Fallot TOF with pulmonary atresia Pulmonary atresia with intact interventricular septum Tricuspid atresia Double outlet right ventricle Transposition of great arteries with ventricular septal defect and pulmonary stenosis Ebstein’s anomaly of tricuspid valve In DORV and tricuspid atresia, there are also variants with increased pulmonary (..)
BackgroundSevere tricuspid regurgitation (TR) causing cyanosis with patent foramen ovale (PFO) and right-to-left atrial shunting requires a precise diagnosis for optimal therapy. Tricuspid valve prolapse (TVP) can lead to TR and is sometimes overlooked, especially in complex cases with factors like pulmonary hypertension (PH).
In Ebstein’s anomaly, there is downward or apical displacement of posterior and septal tricuspid leaflets. The anterior leaflet is not displaced, but is elongated to meet the other leaflets, so that when it closes, a loud sound, tricuspid sound, is produced, which is called as the sail sound.
Lemarchand et al 1 address an everyday question in the echocardiography laboratories about the reliability of systolic pulmonary artery pressure (sPAP) estimation in cases of severe tricuspid regurgitation (TR). As the tricuspid orifice becomes larger and non-restrictive, the convective component.
Objectives The estimation of systolic pulmonary artery pressure (sPAP) by transthoracic echocardiography (TTE) is challenging in patients with severe tricuspid regurgitation (TR). The study aimed to determine the reliability of the assessment of sPAP by TTE in this population.
Echocardiography allows estimation of right ventricular (RV) systolic pressure by adding the estimated right atrial pressure (RAP) to the systolic pressure gradient between the RV and right atrium (RA) calculated from the tricuspid regurgitant (TR) Doppler velocity.
Prognostic impact of severe tricuspid regurgitation (TR) in patients with atrial functional mitral regurgitation (AFMR). Abstract Aims Tricuspid regurgitation (TR) is often seen in patients with atrial functional mitral regurgitation (AFMR).
Introduction Isolated tricuspid valve surgery (TVS) may be associated with high morbidity and mortality. It was associated with ECHO-derived right ventricular (RV) free wall strain and RHC-derived RV systolic and diastolic as well as mean pulmonary pressures. respectively, p<0.05).
Abstract Aim Functional or secondary tricuspid regurgitation (STR) is the most common phenotype of tricuspid regurgitation (TR) with atrial STR (ASTR) and ventricular STR (VSTR) being recently identified as two distinct entities. ASTR vs. VSTR) are lacking. Patients not matching these criteria were classified as VSTR.
FAT in middle-aged and old adult patients was more likely to originate from the crista terminalis, tricuspid annulus, non-coronary cusp, and para-His. Young adults had a higher proportion of FAT originating from the superior vena cava and pulmonary veins. After a mean follow-up of 47.2 months, FAT recurred in 57 patients.
Pulmonary arterial hypertension related to congenital heart disease as a paradigm of complexity Pulmonary arterial hypertension related to congenital heart disease (PAH-CHD) really represents a paradigm of complexity.
(maybe not seen well on these echo-loops) The CW doppler at the tricuspid valve showed a maximum TR velocity of 2,55m/s with a TRP gradient of 26mmHg. large ASD, partial anomalous pulmonary venous return, significant tricuspid regurgitation, carcinoid valvular disease, etc,) 2) Conditions causing pressure overload of the RV. (E.g
Pulmonary arterial hypertension (PAH) is characterized by increased pulmonary vascular resistance, imposing overload on the right ventricle (RV) and imbalance of redox state. PAH induction was implemented by a single dose of MCT (60 mg/kg i.p.). Treatment with SFN (2.5 mg/kg/day i.p.)
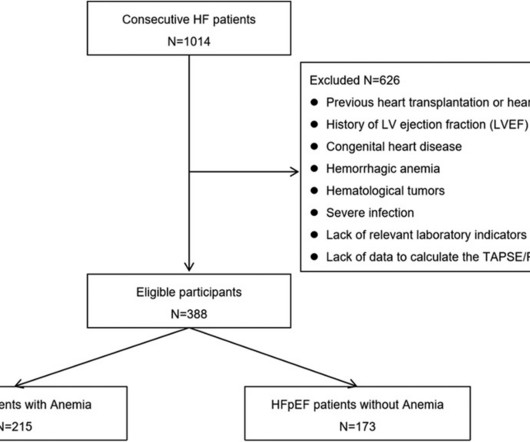
The level of hemoglobin (Hb) had a weak negative linear correlation with NT-pro-BNP (log-transform, r = 0.30, P < 0.0001) and a positively correlation with the tricuspid annular plane systolic excursion (TAPSE)/pulmonary arterial systolic pressure (PASP) ratio (r = 0.44, P < 0.0001).
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It Pulmonary veins have been the primary target for ablation for many years, yet the success rates remain inconsistent. But, we rarely dispute it , & ask which atrium dilates more in AF ? Let us see few factors. References Nil ,
Objective This study assessed the long-term effects of triple therapy with prostanoids on patients with pulmonary arterial hypertension associated with congenital heart disease (PAH-CHD), as there is limited information on the safety and efficacy of this treatment approach.
D-Transposition of the great arteries (TGA) is a rare congenital heart defect where the pulmonary artery originates from the left ventricle (LV) and the aorta from the right ventricle (RV).
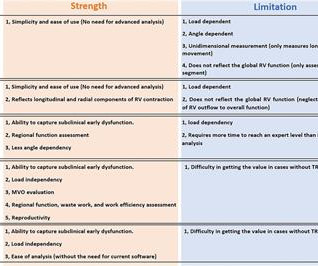
Specifically, “strain”, “RV-pulmonary arterial (PA) coupling”, and “RV myocardial work” are newly applied methods for RV function assessment, a few of which are designed to surmount the load dependency by taking into account the afterload on RV. Recently, novel echocardiographic methods for improved RV assessment have been developed.
In repaired tetralogy of Fallot (rTOF), the septal anatomical isthmuses (AI), 3, between the ventricular septal defect (VSD) and pulmonary annulus, and 4, between the VSD and tricuspid annulus, are important ventricular tachycardia (VT) substrates when slow conducting.
Moreover, pulmonary artery pressures were ameliorated (estimated systolic pulmonary artery pressure: from 47.2±15.8 However, right heart dysfunction as well as the proportion of patients with severe tricuspid regurgitation remained unchanged. ±15.8 ±15.1 mm Hg, p value: 0.0079). to 84.7%) and 74.6% (95% CI 65.9%
Tricuspid valve replacement was performed in 26 (53%) patients including 19 (73%) cases of combined pulmonary valve replacement. Results Out of 43 (16%) consecutive patients with severe CHD and liver metastases of midgut NETs, 79% presented with right-sided heart failure.
Crochetage sign on ECG in ASD ECG in ASD with severe pulmonary hypertension: Tall R’ in V1, ST depression in inferior leads and V2-V5, and T inversion in inferior leads and V1-V6 are seen. All these features together in a cyanotic congenital heart disease is characteristic of tricuspid atresia.
To confirm the efficacy and safety of extra pulmonary vein (PV) ablation, patients were categorized into two groups: those undergoing pulmonary vein isolation (PVI) alone and those receiving additional ablation. Methods Data from early commercial use across seven European centers were collected in a registry.
Methods and Results This case report discusses a 65-year-old man who had previously undergone pulmonary vein isolation (PVI) and cavo-tricuspid isthmus ablation for atrial fibrillation before ASD closure, respectively. He developed atrial tachycardia (AT) and underwent catheter ablation.
IVC diameter correlated to pulmonary arterial (PA) pressure (R=0.347, p<0.001) and body surface area (BSA) (R=0.424 p<0.001). In multivariable Cox regression only IVC diameter (p<0.001), presence of tricuspid regurgitation (p=0.02) and NYHA class III/IV (p<0.001) independently predicted ADHF rehospitalisation within 1 year.
And that will be the approximate level of the tricuspid valve, the reference point for measuring right atrial pressure. In right atrial tracing, this occurs at the time of right ventricular contraction, with bulging upwards of the tricuspid valve. The Y descent is shallow in tricuspid stenosis, and absent in cardiac tamponade.
The tricuspid valve is the right atrioventricular valve. The pulmonary semilunar valve is between the right ventricle and the pulmonary trunk. Several major arteries and veins include: The pulmonary artery transports blood with low levels of oxygen and high levels of carbon dioxide to the lungs.
Patients with IL-6 concentrations cut-off point showed a significantly higher time of STEMI, GOT, higher pulmonary arterial pressure, and longitudinal tracking of left atrial diameter.
The usefulness of JVP in a cardiac emergency like acute pulmonary embolism may appear superfluous. However, tricuspid annular motion is independent of the diastolic relaxation properties of RV. One such thought is described in this animation. Please go to the full-screen view and freeze the video to read the text.
Some of the other useful parameters are mitral E velocity deceleration time, changes in mitral inflow with Valsalva maneuver, mitral L velocity, isovolumic relaxation time, left atrial maximum volume index, pulmonary vein systolic/diastolic velocity ratio, color M-mode Vp and E/Vp ratio.
This suggests that there is pulmonary hypertension and thus possibly RVH. Severe tricuspid regurgitation. --The The estimated pulmonary artery systolic pressure is 31 mmHg + RA pressure. That condition is tricuspid stenosis, which is rare. There is, however, a very peaked P wave in lead II (a "peaked P pulmonale").
The RFCs were much more successful at classifying murmurs from the pulmonary and tricuspid valves (AUROC = 0.83 All RFC models were evaluated using the area under their receiver operating characteristic curves (AUROCs). and 0.78, respectively) when compared with the aortic and mitral valves (AUROC = 0.72 and 0.65, respectively).
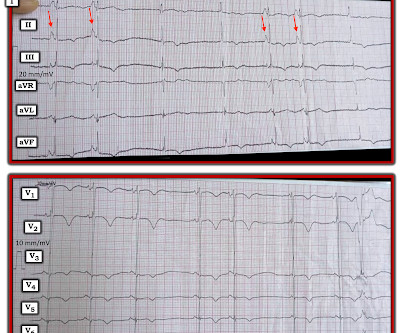
Perhaps the patient has pulmonary hypertension and/or tricuspid regurgitation? RED arrows show what looks to be sinus P waves that are HUGE !!!! consistent with RAA (which is consistent with this patient’s underlying heart disease.
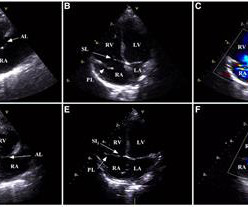
The aorta, right ventricular outflow tract and pulmonary artery up to its bifurcation is imaged in the upward angulation shown in the left panel. Colour flow shows the flow in pulmonary artery. Apical four chamber view shows all four cardiac chambers, mitral and tricuspid valves, and the septa.
We are blessed with 4 heart valves – 2 on the left side which are known as the mitral and aortic valves and 2 on the right side – the tricuspid and pulmonary valves.
Linear mixed models were used to evaluate the predictive value of preoperative echocardiographic parameters on the longitudinal distribution of the 6minute walking test.ResultsPreoperative exercise tricuspid annular plane systolic excursion (TAPSE)/PA systolic pressure strongly correlated with the longterm 6minute walking test (r=0.81,P<0.01).
ABSTRACT Background The impact of tricuspid regurgitation (TR) on the outcomes of pulmonary vein isolation (PVI) for atrial fibrillation (AF) remains unclear.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content