This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
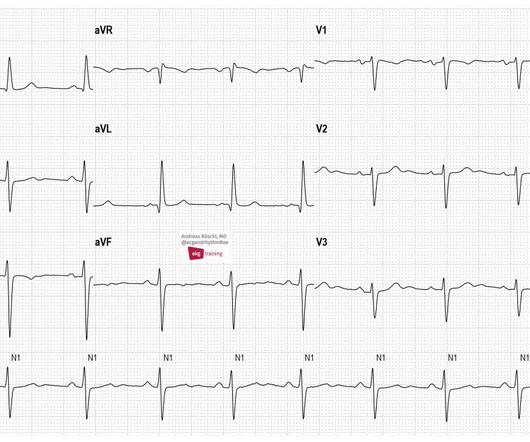
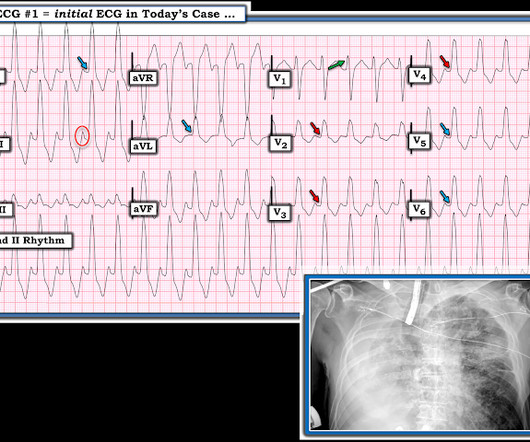
These are typical ECG changes that may indicate a pulmonary embolism. The patient has an acute pulmonary embolism. Sinus tachycardia may be present in acute pulmonary embolism. We see a sinus rhythm with left anterior fascicular block (LAFB) and conspicuous T-wave inversions in the inferior leads and in V1-V6.
Then I always look to see if the initial deflection of the QRS has a lot of voltage change per change in time (seen in tachycardias that are initiated from above the ventricle because the propagate through fast conducting purkinje fiber. Tachycardia exaggerates ST Elevation in LBBB and Paced rhythm 5. Pacemaker mediated tachycardia!
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Bedside ultrasound showed volume depletion and no pulmonary edema. SVT with aberrancy?
Distribution Variance of Focal Atrial Tachycardia Foci and Long-Term Outcomes After Ablation. ABSTRACT Introduction The distribution of the origin of focal atrial tachycardia (FAT) in patients with different ages have not been clearly elucidated. After a mean follow-up of 47.2 months, FAT recurred in 57 patients.
These are typical ECG changes that may indicate a pulmonary embolism. The patient has an acute pulmonary embolism. Sinus tachycardia may be present in acute pulmonary embolism. Wee see a SR with LAFB and conspicuous T-wave inversions in the inferior leads and in V1-V6. ECG 2 was taken from the same patient 1 year earlier.
On the monitor patient had wide-complex tachycardia. Differential is ventricular tachycardia versus supraventricular tachycardia with aberrancy versus sinus tachycardia with a aberrancy. After the patient was stabilized with supportive care, the heart rate gradually slowed, confirming sinus tachycardia.
Electroanatomic mapping guides complex atrial tachycardia ablations; however, challenges may emerge after pulmonary vein isolation. 3D mapping systems can reveal the mechanism of tachycardia and critical areas that need to be ablated.
CT of the chest showed no pulmonary embolism but bibasilar infiltrates. Even with tachycardia and a paced QRS duration of ~0.16 (And of course Ken's comments at the bottom) An elderly obese woman with cardiomyopathy, Left bundle branch block, and chronic hypercapnea presented hypoxic with altered mental status. She was intubated.
The ECG in Figure-1 — was obtained from a middle-aged woman with positional tachycardia and diaphoresis with change of position from suprine to sitting. My THOUGHTS on the ECG in Figure-1: The rhythm is sinus tachycardia at ~105/minute ( ie, The R-R interval is regular — and just under 3 large boxes in duration ).
It shows sinus tachycardia with right bundle branch block. Taking a step back , remember that sinus tachycardia is less commonly seen in OMI (except in cases of impending cardiogenic shock). In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonary embolism. Both were wrong.
Superior vena cava (SVC) can be the site of origin for both non-pulmonary vein trigger for atrial fibrillation and atrial tachycardia (AT). The mechanism of ATs arising from the SVC is commonly focal discharge.
Although increasing evidence supports substrate-based ablation strategies targeting extra-PV sources, reliable endpoints during CA beyond pulmonary vein (PV) isolation are not well established. Radiofrequency catheter ablation (RFCA) for persistent atrial fibrillation (AF) is associated with suboptimal long-term outcomes.
Introduction Multiple abnormal electrocardiographic findings have been documented in patients experiencing acute pulmonary embolism. Although sinus tachycardia is the most commonly encountered rhythmic disturbance, subsequent reports have highlighted other findings.
Scimitar syndrome is a rare congenital heart defect characterized by a triad: anomalous arterial supply, pulmonary hypoplasia of the right lung, and anomalous right pulmonary venous return to the inferior vena cava, resembling the curved Middle Eastern sword, or scimitar.
A 77-year-old male with a history of two catheter ablation procedures, including pulmonary vein isolation and superior vena cava (SVC) isolation, presented with symptomatic palpitations. A twelve-lead electrocardiogram revealed atrial tachycardia (AT) with a cycle length of 240 ms.
There was no pulmonary edema or hypoxia. Here was his initial ECG: Regular Wide Complex Tachycardia. Blood pressure was 180/80. Cardiac Echo showed excellent hyperdynamic function. The computer read the QRS duration as 160 ms. However, many toxins do not show up on tox screens. Sinus --Irregularly irregular?
Epicardial Marshall bundle (MB) are frequently utilized in left atrial tachycardias (LATs) post atrial fibrillation (AF) ablation with pulmonary vein isolation and substrate modification.
Left atrial low-voltage areas (LVAs) are an important arrhythmogenic substrate that can act as an anatomical barrier of reentrant atrial tachycardias (ATs). However, ATs are not always induced in patients with LVAs, and identification of areas with a slow conduction velocity (CV) may help us predict the occurrence of ATs.
I see the following: There is sinus tachycardia ( upright P wave with fixed PR interval in lead II ) — at the rapid rate of ~130/minute. Sinus Tachycardia and RAD — as already noted above. PEARL # 2: In the absence of associated heart failure ( cardiogenic shock ) — sinus tachycardia is not a common finding in acute MI.
Both atria develop from a combination of the primitive atrium, sinus venous, and pulmonary veins.It In all probability, this dilation is a form of atrial tachycardia and atrial cardiomyopathy. In contrast to other tachycardias, with atrial fibrillation (AF), the focus is often speculative, and ablation attempts are made accordingly.
Treatment of persistent AF may require additional substrate modification beyond simple pulmonary vein (PV) isolation. However, atrial tachycardias (ATs) may develop in a portion of such patients, and mapping and ablating these can be challenging.
He was in acute distress from pulmonary edema, with a BP of 180/110, pulse 110. He had diffuse crackles on exam and B-lines on chest ultrasound, and chest x-ray also confirmed pulmonary edema. Here is his ED ECG: There is sinus tachycardia. The hypertension alone is the likely etiology of the pulmonary edema.
Ablation of regions demonstrating spatiotemporal dispersion (SD) has been demonstrated as an alternative strategy beyond pulmonary vein isolation in patients with persistent atrial fibrillation. Occurrence of atrial tachycardia (AT) following ablation remains a limitation of this approach.
Pulse field ablation (PFA) using a pentaspline catheter is an effective and safe treatment method for pulmonary vein isolation (PVI) in patients with atrial fibrillation (AF).1,2 We present a case of a macro-reentrant atrial tachycardia in the lateral right atrium (RA) treated by PFA using a pentaspline catheter.
They had already cardioverted at 120 J, then 200 J, which resulted in the following: Ventricular Tachycardia They then cardioverted at 200 J which r esulted in the same narrow complex rhythm shown above, at 185 beats per minute. This would treat both SVT or sinus tachycardia. I suggested esmolol if the heart rate did not improve.
Besides single-shot PFA devices for pulmonary vein isolation (PVI), point-by-point PFA is also gaining importance due to many possible applications. Data on the use is sparse, especially for atrial tachycardia (AT). Pulsed-field ablation (PFA) is becoming increasingly relevant in the field of electrophysiology.
Here is his ECG: Original image, suboptimal quality Quality improved with PM Cardio digitization The ECG is highly suggestive of acute right heart strain, with sinus tachycardia, S1Q3T3, and T wave inversions in anterior and inferior with morphology consistent with acute right heart strain. Moreover, there is tachycardia.
Multifocal Atrial Tachycardia 2. MAT almost always occurs in one of 2 common clinical scenarios : i ) Severe pulmonary disease ( ie, COPD, long-term asthma; pulmonary hypertension ) ; or , ii ) Acutely ill patients with multisystem disease ( ie, patients with sepsis; shock; electrolyte and/or acid-base disorders ).
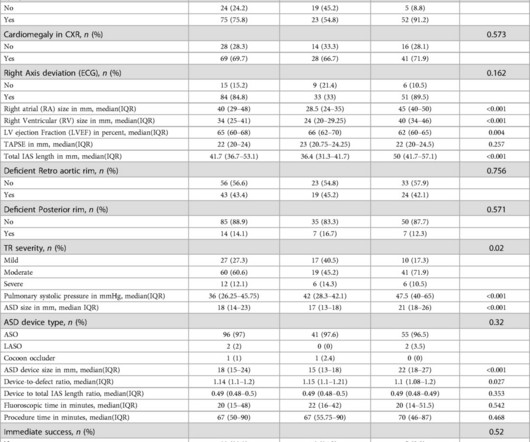
Patients in Group 2 had greater pulmonary artery systolic pressure than those in Group 1 (p-value<0.001). and paroxysmal supraventricular tachycardia (SVT) (5.3%), respectively. The most common symptoms in adults were easy fatigability and dyspnea (63.2% Overall, 88.9% and Group 2: 2.5 (IQR IQR 22.5); P-value=0.111].
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
She had acute pulmonary edema on exam. On arrival, lung ultrasound confirmed pulmonary edema (B lines). Conventional algorithm interpretation: SINUS TACHYCARDIA ABNORMAL RHYTHM ECG Confirmed by over-reading physician Transformed ECG by PM Cardio: PM Cardio interpretation: OMI with Low Confidence Dr.
Given the rapid adoption of pulse field ablation (PFA), there is interest in uses beyond pulmonary vein isolation. Here, we describe a case of incessant atrial tachycardia (AT), in which PFA resulted in short-term arrhythmia suppression but tachycardia recurred and lesion size regressed on interval mapping.
Vein of Marshall ethanol ablation (VOM-EA) as an adjunct to pulmonary vein isolation (PVI) has been reported to improve freedom from atrial fibrillation (AF) and atrial tachycardia (AT).
She was noted to be in heart failure, with hypotension and tachycardia. Echocardiography demonstrated severe calcific mitral stenosis with pulmonary hypertension. With decompensated heart failure and adequate prior anticoagulation, the patient underwent direct current synchronised cardioversion for her arrhythmia.
Methods This study enrolled 233 PeAF patients undergoing pulmonary vein isolation and linear ablation including an MI, roof line, and cavotricuspid isthmus ablation. During the follow-up, 113 (64.9%) RF group patients were free from AF/atrial tachycardia compared to 41 (82.0%) EIVOM group patients (log-rank p = .045). 0.78, p = .006).
Pulsed field ablation (PFA) is a reliable treatment modality in the pulmonary vein (PV) antra and the left atrial posterior wall (LAPW), but lesion durability in other atrial segments may be less optimal with the current PFA systems.
Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. The estimated pulmonary artery systolic pressure is 37 mmHg + RA pressure. QTc was 374, and the formula value was quite high, consistent with LAD occlusion.
NOTE: For more on ECG recognition of RVH and/or pulmonary hypertension ( re the qR pattern in lead V1 ) — See ECG Blog #234 and Blog #248. Because of this, it is uncommon to see sinus tachycardia with a prolonged PR interval. This is precisely what we see in Figure-6. Unfortunately — I lack this information.
The safety and efficacy of Pulsed-field ablation (PFA) for pulmonary vein isolation (PVI) using a five spline, multielectrode, PFA catheter has been well studied. There is little data assessing the outcomes following anterior mitral line (AML) creation, for substrate modification or treatment of atrial tachycardia (AT), with this catheter.
Smith interpretation: This is highly likely to be due to extreme right heart strain and is nearly diagnostic of pulmonary embolism. It is of course pulmonary embolism. No d-dimer or CT pulmonary angiogram was done when they discovered that she had normal coronary arteries. Junctional tachycardia? ).
In addition to single-shot devices mainly used for pulmonary vein isolation, focal PFA may provide a treatment option that increases the versatility of the technique. Pulsed field ablation (PFA) has become increasingly important in the treatment of cardiac arrhythmias.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content