This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Patients with acute pulmonary embolism (PE) have a wide spectrum of clinical presentations, from incidental findings to suddencardiacdeath. Here, we propose an algorithm where the role of the Pulmonary Embolism Response Team (PERT) is reinforced. PROSPERO registration number: CRD42024493303.
However, the cause and risk factors for mortality remain uncertain.MethodsThis retrospective, singlecenter study identified children with primary and secondary pulmonary vein stenosis through a cardiac catheterization database. All patients underwent cardiac catheterization, with 45 (80%) undergoing at least 1 interventional procedure.
This specialized and complex procedure is the optimal treatment for replacing a diseased aortic valve in adolescents and adults with the patient’s own living pulmonary valve—a mirror image of a normal aortic valve—resulting in improved long-term life expectancy, unlike mechanical or tissue valve replacements.
One is ventricular septal defect, second is overriding aorta, third is pulmonary stenosis, usually right ventricular outflow tract stenosis and associated right ventricular hypertrophy. Pulmonary stenosis, which is usually right ventricular outflow tract stenosis. This will almost invariably result in severe pulmonary regurgitation.
It is crucial for every medical physician to recognize patients who are at risk of suddencardiacdeath due to their underlying medical condition. It is crucial for every medical physician to recognize patients who are at risk of suddencardiacdeath due to their underlying medical condition.
Background:Epicardial patch defibrillators (EPDs) were commonly implanted in the 1990s for secondary prevention of suddencardiacdeath. This case highlights such a scenario.Case:A 75-year-old female with a history of cardiac arrest 30 years ago presented with shortness of breath and left leg swelling.
Brugada syndrome is thought to account for about one fourth of suddencardiacdeaths in individuals with structurally normal heart. Even though mutations in other channels have been described in Brugada syndrome, only those in SCN5A gene are considered to be definitely disease causing. mV or R/q ≥ 0.75.
Further ultrasound showed no B-lines (no pulmonary edema). HCM is estimated to occur in ~1 in 500 young adults , making it among the most common inherited cardiac disorders. The heart rate is too fast for this poor filling. Preload must be increased and the heart rate slowed in order to allow more LV filling. If so — WHO to screen?
What caused these 729 deaths (filtered out of 29000 deaths) I understand physical autopsy could not be done in majority of deaths (Even in witnessed , in hospital deaths). Is it suddencardiacdeath ? Is it sudden “non cardiac ” death ? So, the question remains.
No family history of suddencardiacdeath, cardiomyopathy, premature CAD, or other cardiac issues. CT angiogram chest: no aortic dissection or pulmonary embolism. Serial chest xrays: progressive bilateral pulmonary edema. No similar symptoms in the past. No further troponins were measured.
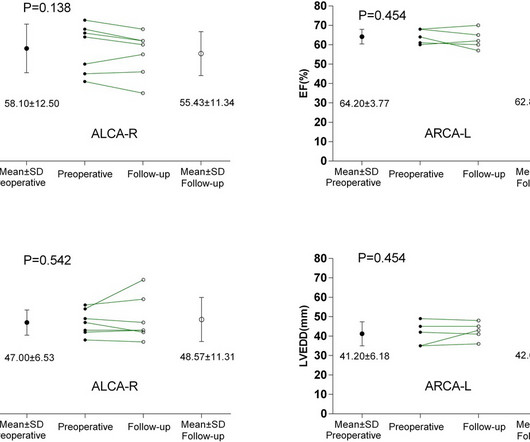
BackgroundAnomalous aortic origin of a coronary artery (AAOCA) is associated with an increased risk of myocardial ischemia and suddencardiacdeath. The incidence of postoperative cardiac-type symptoms (angina, syncope or dyspnea) was higher in ALCA-R patients compared to ARCA-L patients.
BackgroundThe Anomalous Origin of the Right Coronary Artery from the Left Coronary Sinus (ARCA-LCS) is a rare congenital cardiac condition where the right coronary artery emerges from the left sinus instead of the right coronary sinus of Valsalva. Cranial magnetic resonance imaging and magnetic resonance angiography showed no abnormalities.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content