This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
ABSTRACT Introduction Pulmonary vein (PV) restenosis develops with reported incidence rates of up to 50%. The stenosis was treated with a stent. years later he presented with an in-stent restenosis that was successfully treated with a stent-in-stent strategy. The stenosis was treated with a stent.
Due to the implantation technique, left pulmonary artery (LPA) stents represent a relative contraindication to Venus P-valve. 3/16 (18.7%) patients underwent Venus P-valve implantation with LPA stents. 3/16 (18.7%) patients underwent Venus P-valve implantation with LPA stents.
Some of the late-breaking topics that will be covered include transcatheter aortic valve replacement (TAVR), peripheral artery disease (PAD), and pulmonary embolism (PE): Impact of Age on Procedural Timing for Asymptomatic Severe Aortic Stenosis: Results from the Early TAVR Trial The PERFORMANCE II Trial: A Prospective Multicenter Single Arm Investigation (..)
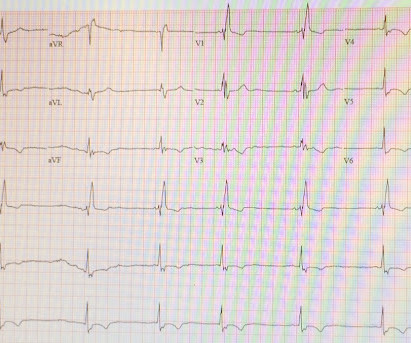
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. He was in acute distress from pulmonary edema, with a BP of 180/110, pulse 110. The hypertension alone is the likely etiology of the pulmonary edema.
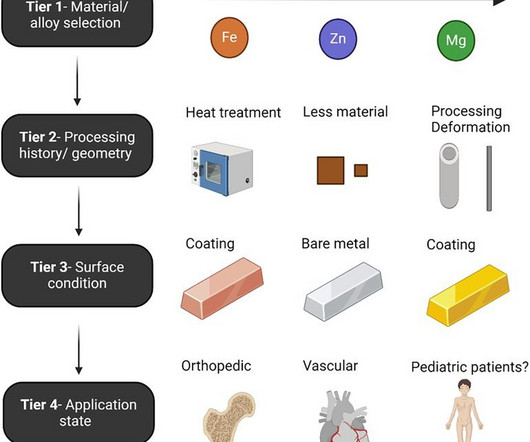
The past five years have yielded impressive advancements in fully absorbable metal stent technology. Nowhere is the need for fully absorbable metal stents greater than in patients experiencing vascular anomalies associated with congenital heart disease (CHD).
Stent performance was assessed.ResultsWe identified 28 patients (67.8% Stenotic lesions included 16 branch pulmonary arteries, 9 aortic isthmus, 2 right ventricular outflow tracts, and 1 Glenn anastomosis. The procedures mostly used 7 Fr sheaths for stents on 6, 7, and 8 mm balloons and 8 Fr sheaths for 9, 10, 12 mm balloons.
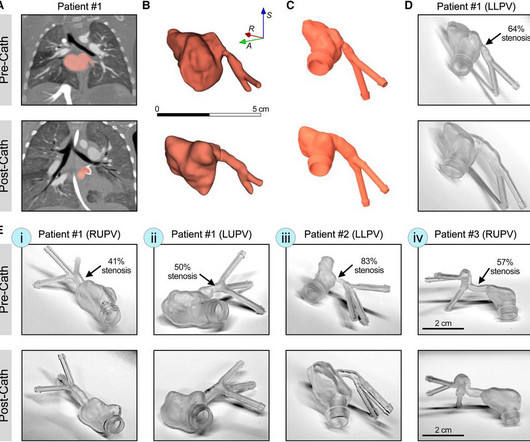
IntroductionPrimary pulmonary vein stenosis (PVS) is a rare congenital heart disease that proves to be a clinical challenge due to the rapidly progressive disease course and high rates of treatment complications. These 3D reconstructions were 3D printed using a clear resin ink and used in a benchtop experimental setup.
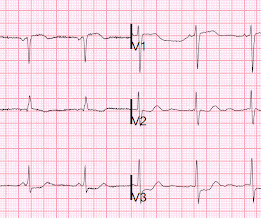
It is of an elderly woman who complained of shortness of breath and had a recent stent placed. Ken (below) is appropriately worried about pulmonary embolism from the ECG. What I had not told him before he made that judgement is that the patient also had ultrasound B-lines of pulmonary edema. What do you think?
Treatment for infants who have severe pulmonary arterial hypertension (PAH) is sometimes limited. Because they haven't physically matured, a procedure could increase the risk of serious complications, including failure of the heart's right ventricle.
BACKGROUND:Covered stent correction (CSC) of a superior sinus venosus atrial septal defect is an alternative to surgery in selected patients, but anatomic variation means that assessment for CSC requires a 3-dimensional anatomic understanding. Circulation: Cardiovascular Interventions, Volume 17, Issue 12 , Page e013964, December 1, 2024.
Our Interventional Cardiology Fellowship Program offers a unique opportunity for fellows to immerse themselves in high-volume centers and experience complex procedures such as angioplasties, stent placements, and Chronic Total Occlusion (CTO) interventions. Requirements This specialty requires a background in internal medicine or pediatrics.
BackgroundThe modified Blalock‐Taussig‐Thomas shunt is the gold standard palliation for securing pulmonary blood flow in infants with ductal‐dependent pulmonary blood flow. Journal of the American Heart Association, Volume 12, Issue 23 , December 5, 2023.
The combined and matched subgroups were pulmonary artery stenting (Stent PUL ), aorta angioplasty (Plasty AO ), pulmonary artery angioplasty (Plasty PUL ), or a combination of the latter two (Plasty). The decrease of AK BW and DAP BW in the Stent PUL and Plasty PUL subgroups was not statistically significant.
BackgroundThe VenaTech Convertible Vena Cava Filter (VTCF) is a device designed for insertion into the inferior vena cava (IVC) to prevent life-threatening pulmonary embolism (PE).
Chance of precipitating a cyanotic spell are more when pulmonary angiography is attempted through the already narrow right ventricular outflow tract. initial shunt surgery is an option to allow the pulmonary artery branches to grow in size and for a later complete repair of tetralogy of Fallot [1]. If McGoon’s ratio is below 0.8,
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. Does this change your interpretation?
The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented. I wonder if this patient had pulmonary disease? For more on ECG findings in pulmonary disease — Check out My Comment in the May 31, 2024 post in Dr. Smith's ECG Blog ). All intervals ( PR-QRS-QTc ) are normal.
In SCAPE (sympathetic crashing acute pulmonary edema), Emergency providers seem now to regularly give high dose NTG, but when the BP is 170/105 in a patient who is not crashing, we often fail to give something to lower afterload. __ Here are some Images: The red circle shows the LAD coursing down the anterior interventricular sulcus.
IntroductionThe 2015 American Heart Association Guidelines recommended mechanical thrombectomy with stent‐retriever devices. Compared with 2012‐2014, the 2015‐2019 cohort showed increased odds of ICH and shock while the odds of DVT, pulmonary embolism, pneumonia, and UTI were significantly lower.
Xray was consistent with pulmonary vascular congestion. Previously placed stents in the LAD (multiple) and mid circumflex and patent Formal echocardiogram: Normal left ventricular size and wall thickness. Bedside echo showed no evidence of reduced EF, no signs of right heart strain, no regional wall abnormality.
On day 3 of hospitalization she underwent coronary angiography, revealing a 95% lesion in the mid-LAD which was stented. A new right bundle branch block in a sick patient with chest pain and/or shortness of breath is a worrisome finding concerning for LAD occlusion or significant pulmonary embolism.
There was some pulmonary edema. Perusal of her charts revealed that she had an LAD stent that was very close to the ostium of the circumflex. They texted me the following ECGs, which I viewed in the shade of a pine tree on a glorious sunny snowy landscape. AT&T surprised me with their reach. This is her ECG 1.5
The patient had been on a long drive, suggesting possible pulmonary embolism (this was unlikely given absence of tachyardia, hypoxia, or any other feature of PE), so we sent a d dimer. [We It was opened and stented with a door to balloon time of about 120 minutes (this is long for STEMI, but very short for a high risk Non STEMI).
No signs for aortic dissection or pulmonary embolus. --"Results were discussed with the ordering physician. INTERVENTION * Successful angioplasty and stenting (drug eluting) of the mid LAD * Successful angioplasty of the ostial 1st diagonal Learning points: 1. A CT Coronary angiogram was ordered. LAD plaque with 0-25 percent stenosis.
Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. A majority of patients with MAT have longstanding pulmonary disease. Rather than antiarrhythmic medication — optimizing pulmonary function is the best treatment approach. To our knowledge, the patient did well.
As a result, healthcare faces rising expenses from frequent emergency room visits, lengthy hospital stays, costly procedures like stent placements and bypass surgeries, as well as the long-term management of chronic conditions like heart failure (HF). These costs represent a massive portion of total health expenditures.
February 2024 FDA Approvals: Innovations in Cardiovascular Interventions XACT Carotid Stent System (Approved: 02/07/2024) This approval expands the indications to be used during a Transcarotid Artery Revascularization (TCAR) procedure to prevent future strokes.
Outcome In the EVAR group, 47 patients (95.92%) were successfully implanted with overlapping stents, and 2 patients died in the perioperative period. In the TAAR group, 12 patients (92.31%) were successfully revascularized and 1 patient died in the perioperative period.
INFINITY-SWEDEHEART Trial: This randomized controlled trial, developed by Elixir Medical, compared the DynamX® Coronary Bioadaptor System with the Resolute Onyx drug-eluting stent.
On his physical examination, cardiac and pulmonary auscultation was completely normal. Bi-phasic scan showed no dissection or pulmonary embolism. The lesion was successfully stented. He has 40 packs-year of smoking history. There was no premature cardiovascular diseases or sudden death in his family.
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. This was stented. Medics stated that he had not been taking his clopidogrel for 2 weeks. He appeared to be in shock. Here is his ED ECG: There is obvious infero-posterior STEMI. After pacing, there was no recurrence of Torsades.
Here is another proven left main occlusion in a young woman who presented with sudden pulmonary edema, had this ECG recorded, then arrested and was resuscitated after 30 minutes of CPR: This has sinus tachycardia with RBBB and LAFB, and STE in V2-V6 as well as I, aVL This pattern could just as easily be seen in LAD occlusion.
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
A completely blocked artery is located, a wire is inserted through it, the clot is sucked, the narrowing is widened with a balloon, and then a stent (stainless steel wire mesh) is placed to maintain consistent flow. Coronary angiography is performed under local anesthesia using the right arm without any cuts.
This study reports a rare case of concurrent AMI and pulmonary thromboembolism in a patient diagnosed with pancreatic cancer.Case presentationA 70-year-old woman presented with acute chest pain and ST-segment elevation myocardial infarction, prompting immediate percutaneous coronary intervention (PCI) with the deployment of a drug-eluting stent.
thoracic aortic dissection, thoracic aortic aneurysm, and/or type B intramural hematoma) as well as the presence of T1ELs or T2ELs.ResultsReoperation was more common in the T1EL group (n=4; 57%) than in the T2EL group (n=2; 29%); also, reintervention for stenting of the thoracic endovascular graft was more frequent in the T1EL group (4 vs. 1).
August 2024 Approvals Minima Stent System (P240003) (Approval Date: August 28, 2024) The Minima Stent System is an expandable cobalt-chromium metal mesh tube to reopen blood vessels in neonates, infants, and children with Coarctation of the Aorta and Pulmonary Artery Stenosis, specifically designed to expand as younger patients grow.
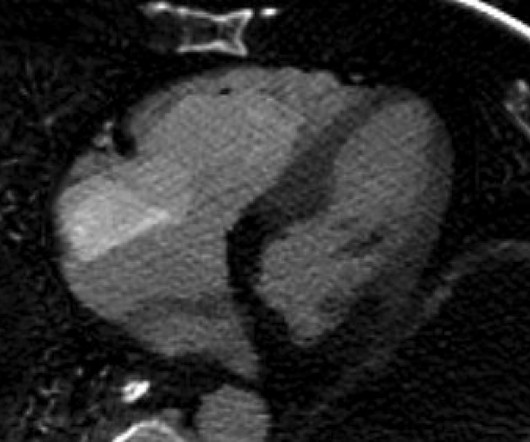
It did not show pulmonary embolism or intra-abdominal pathology, but it did show this: See the dark area at the bottom of the image? There was no pulmonary embolism. With the severe acidosis and absence of ST elevation, they felt there was more likely to be a non-cardiac etiology of his presentation.
His initial high sensitivity troponin I returned at 1300 ng/L and given that his cardiac workup was otherwise unremarkable, a CT was obtained to evaluate for pulmonary embolism and aortic aneurysm or dissection but this too was unrevealing. Also: electrical instability, pulmonary edema, or hypotension. Another EKG was also obtained.
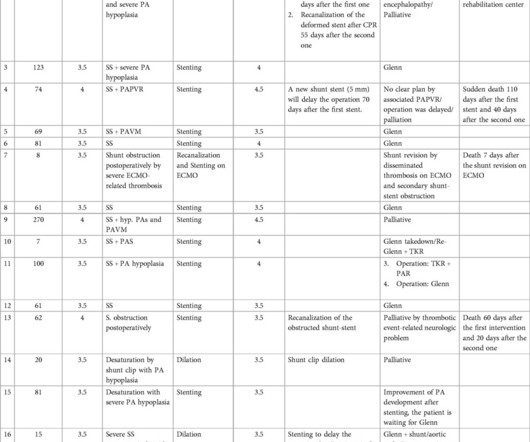
In-stent thrombosis, a late complication, occurred in four patients; two of these had impaired anticoagulation, including extracorporeal membrane oxygenation (ECMO)-related causes, while the other two, who were on aspirin, had multiple stents within the shunt, one of whom experienced sudden death.
No pulmonary embolism is identified. First obtuse marginal also had an 80% stenosis and was stented. While in the ED, patient's pain worsened to previous severity of 6/10 pain and improved to 3/10 on NTG drip. CT Angio Chest IMPRESSION 1. No thoracic aortic hematoma, aneurysm or dissection.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content