This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Some of the late-breaking topics that will be covered include transcatheter aortic valve replacement (TAVR), peripheral artery disease (PAD), and pulmonary embolism (PE): Impact of Age on Procedural Timing for Asymptomatic Severe Aortic Stenosis: Results from the Early TAVR Trial The PERFORMANCE II Trial: A Prospective Multicenter Single Arm Investigation (..)
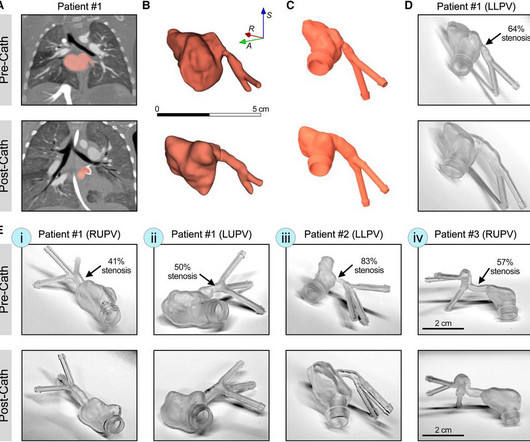
IntroductionPrimary pulmonary vein stenosis (PVS) is a rare congenital heart disease that proves to be a clinical challenge due to the rapidly progressive disease course and high rates of treatment complications. These 3D reconstructions were 3D printed using a clear resin ink and used in a benchtop experimental setup.
ABSTRACT Introduction Pulmonary vein (PV) restenosis develops with reported incidence rates of up to 50%. The stenosis was treated with a stent. years later he presented with an in-stent restenosis that was successfully treated with a stent-in-stent strategy. The stenosis was treated with a stent.
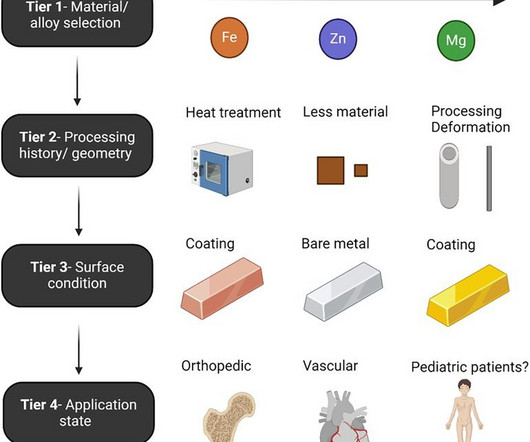
The past five years have yielded impressive advancements in fully absorbable metal stent technology. The desired ultimate ability for such devices to treat a vascular stenosis without long-term device-related complications or impeding future treatment continues to evoke excitement in clinicians and engineers alike.
Chance of precipitating a cyanotic spell are more when pulmonary angiography is attempted through the already narrow right ventricular outflow tract. initial shunt surgery is an option to allow the pulmonary artery branches to grow in size and for a later complete repair of tetralogy of Fallot [1]. If McGoon’s ratio is below 0.8,
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. Does this change your interpretation?
In SCAPE (sympathetic crashing acute pulmonary edema), Emergency providers seem now to regularly give high dose NTG, but when the BP is 170/105 in a patient who is not crashing, we often fail to give something to lower afterload. __ Here are some Images: The red circle shows the LAD coursing down the anterior interventricular sulcus.
LAD plaque with 0-25 percent stenosis. No signs for aortic dissection or pulmonary embolus. --"Results were discussed with the ordering physician. The LAD has moderate 40% ostial-proximal LAD stenosis and severe 90% mid LAD stenosis involving first diagonal branch. --The A CT Coronary angiogram was ordered.
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. The patient had been on a long drive, suggesting possible pulmonary embolism (this was unlikely given absence of tachyardia, hypoxia, or any other feature of PE), so we sent a d dimer. [We
61,62) The interventional community defines occlusive LM disease as >50% by FFR, or ≥75% stenosis,(63) but urgent or emergent intervention on lesions not meeting these thresholds is only imperative if it is a thrombotic lesion and the patient has refractory ischemic symptoms (i.e. and I sent him the above ST vector explanation.
Institutional Coronary Artery Bypass Case Volumes and Outcomes European Journal of Heart Failure October 2023 Makoto Mori 1 Robotic Mitral Valve Repair for Degenerative Mitral Regurgitation The Annals of Thoracic Surgery August 2023 Carlos Diaz-Castrillion 2 Volume-Failure to Rescue Relationship in Acute Type A Aortic Dissections: An Analysis of The (..)
August 2024 Approvals Minima Stent System (P240003) (Approval Date: August 28, 2024) The Minima Stent System is an expandable cobalt-chromium metal mesh tube to reopen blood vessels in neonates, infants, and children with Coarctation of the Aorta and Pulmonary Artery Stenosis, specifically designed to expand as younger patients grow.
No pulmonary embolism is identified. First obtuse marginal also had an 80% stenosis and was stented. While in the ED, patient's pain worsened to previous severity of 6/10 pain and improved to 3/10 on NTG drip. CT Angio Chest IMPRESSION 1. No thoracic aortic hematoma, aneurysm or dissection.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content