This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. He was in acute distress from pulmonary edema, with a BP of 180/110, pulse 110. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! He had no chest pain.
The conventional machine algorithm interpreted this ECG as STEMI. In patients with narrow QRS ( not this patient), this pattern is highly suggestive of acute pulmonary embolism. Answer : Bedside ultrasound! Smith : RV infarct may also have this appearance on ultrasound. Her ECG is shown below: What do you think?
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." He was started on a heparin drip and CTA of the chest was ordered to rule out pulmonary embolism. Unfortunately, there was a long wait and the patient left before being seen by a provider.
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Armstrong et al.)], the presence of such well developed anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
The following ECG was recorded: There is an obvious acute inferior STEMI. Whenever there is inferior STEMI, one should think about Right Ventricular STEMI (RVMI). As 85% of inferior STEMI are due to RCA occlusion [the rest due to occlusion of a "dominant" circumflex (i.e., and STE in lead III > STE in lead II.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. Smith comment: before reading anything else, this case screamed pulmonary embolism to me. The prehospital, ED computer, and final cardiology interpretation was STEMI negative.
This case was posted on the [link] ultrasound site, of which this ECG blog is a part. I refer you to the video case presentation by one of my colleagues, Dr. Rob Reardon (who has, by the way, a fantastic collection of ED ultrasound cases). In this case, the ECG never mimicked a STEMI.
A bedside cardiac ultrasound was recorded: Here is a still image of the echo: The red arrows outline the right ventricle and the yellow arrows outline the left ventricle chamber. It makes pulmonary embolism (PE) very likely. The small LV implies very low LV filling pressures, which implies low pulmonary venous pressure.
She had acute pulmonary edema on exam. Prehospital Conventional algorithm interpretation: ANTERIOR INFARCT, STEMI Transformed ECG by PM Cardio: PM Cardio AI Bot interpretation: OMI with High Confidence What do you think? On arrival, lung ultrasound confirmed pulmonary edema (B lines).
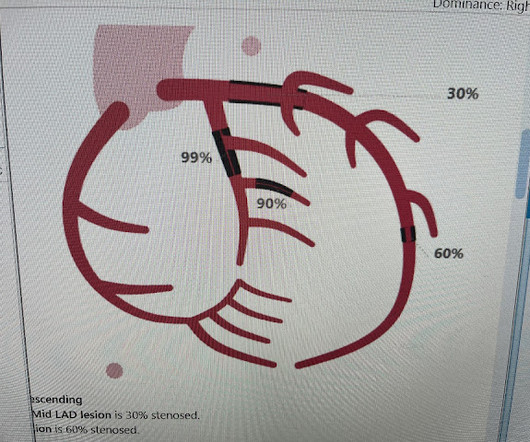
In SCAPE (sympathetic crashing acute pulmonary edema), Emergency providers seem now to regularly give high dose NTG, but when the BP is 170/105 in a patient who is not crashing, we often fail to give something to lower afterload. __ Here are some Images: The red circle shows the LAD coursing down the anterior interventricular sulcus.
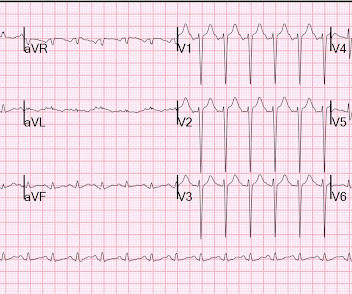
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5
Could this be Septal STEMI (STE in V1 and aVR, with reciprocal ST depression in V4-V6?), In Septal STEMI , transmural ischemia of the septum is recorded by the overlying lead V1 as ST Elevation. Lead III is also on the right and might manifest ST Elevation in Septal STEMI. with ADDED STE in III?
This meets "STEMI criteria" However, there is very high voltage, with a very deep S-wave in V2 and tall R-wave in V4. The morphology is not right for STEMI. My interpretation: LVH with secondary ST-T abnormalities, exaggerated by stress, not a STEMI. This is very good evidence that the ST elevation is not due to STEMI.
To me, this looks like pulmonary edema. A bedside ultrasound was done, with dozens of clips, and was even done with Speckle Tracking. B-line predominance bilateral lungs indicates pulmonary edema. B-line predominance bilateral lungs indicates pulmonary edema. Because we are hypnotized the STEMI paradigm. "If
The morphology of V2-V4 is very specific in my experience for acute right heart strain (which has many potential etiologies, but none more common and important in EM than acute pulmonary embolism). CT angiogram showed extensive saddle pulmonary embolism. Now another, with ultrasound. On epinephrine and norepinephrine drips."
Smith comment: This patient did not have a bedside ultrasound. Had one been done, it would have shown a feature that is apparent on this ultrasound (however, this patient's LV function would not be as good as in this clip): This is recorded with the LV on the right. In fact, bedside ultrasound might even find severe aortic stenosis.
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. CT angiogram chest: no aortic dissection or pulmonary embolism. 24 yo woman with chest pain: Is this STEMI?
This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. If the arrest had another etiology (such as old scar), and the ST elevation is due to severe shock, then it is a type II STEMI. I believe the latter (type II STEMI) is most likely.
Exclusion criteria were age less than 18, SBP less than 100 mmHg, echocardiogram with EF less than 50%, STEMI, pregnancy, and trauma. While sensitivity of this sign is very low — its presence is highly suggestive of longstanding and severe pulmonary disease. Clin Cardiol 22:334-344, 1999 ).
A bedside cardiac ultrasound was normal, with no effusion. and the patient was converted to veno-venous (V-V) ECMO due to persistent pulmonary insufficiency. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease.
Patients with pulmonary embolism or aortic dissection who have normal variant ST elevation are at high risk of being diagnosed with pericarditis when what they have is far more serious!! normal variant, not pericarditis) A Young Man with Sharp Chest pain (normal variant, not pericarditis) 24 yo woman with chest pain: Is this STEMI?
I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Anything that causes pulmonary edema: poor LV function, fluid overload, previous heart failure (HFrEF or HFpEF), valvular disease. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI).
These ECGs were texted to me by one of our previous ultrasound fellows, Will Smoot An elderly male arrived via EMS for acute substernal chest pain with radiation to left shoulder and arm that awakened him from sleep at 0030. No acute infectious prodrome, known pulmonary disease, or recent trauma. No prior similar symptoms or known CAD.
Case continued A bedside cardiac ultrasound revealed grossly preserved left ventricular function, no appreciable wall motion abnormality, pericardial effusion, or obvious valvular abnormality. Also: electrical instability, pulmonary edema, or hypotension. In this case, there was electrical instability (Mobitz II block).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content