This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
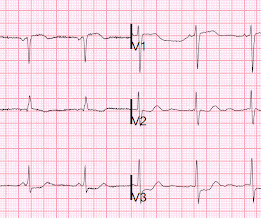
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. He was in acute distress from pulmonary edema, with a BP of 180/110, pulse 110. Is this acute STEMI? Is this an acute STEMI? -- Unlikely!
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion.
In SCAPE (sympathetic crashing acute pulmonary edema), Emergency providers seem now to regularly give high dose NTG, but when the BP is 170/105 in a patient who is not crashing, we often fail to give something to lower afterload. __ Here are some Images: The red circle shows the LAD coursing down the anterior interventricular sulcus.
There was some pulmonary edema. This is typical for subendocardial ischemia, not STEMI, and often means left main ischemia or 3 vessel ischemia. Right sided ECGs are best recorded in the context of inferior STEMI. Because of precordial ST depression, clinicians were also worried about posterior STEMI. This is her ECG 1.5
The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented. The Non-STEMI, which was an OMI, was diagnosed much faster with AI on the ECG than with troponin. I wonder if this patient had pulmonary disease? Then the high sensitivity troponin T returned at 1400 ng/L.
The "criteria" for posterior STEMI are 0.5 Is it STEMI or NonSTEMI? The patient had been on a long drive, suggesting possible pulmonary embolism (this was unlikely given absence of tachyardia, hypoxia, or any other feature of PE), so we sent a d dimer. Patients with ACS and acute pulmonary edema 3. mm STE in one lead.
Xray was consistent with pulmonary vascular congestion. 20% of cases that everyone would call a STEMI have a competely open artery by the time of angiogram 60-90 minutes later. Previously placed stents in the LAD (multiple) and mid circumflex and patent Formal echocardiogram: Normal left ventricular size and wall thickness.
No signs for aortic dissection or pulmonary embolus. --"Results were discussed with the ordering physician. INTERVENTION * Successful angioplasty and stenting (drug eluting) of the mid LAD * Successful angioplasty of the ostial 1st diagonal Learning points: 1. Transient STEMI is at high risk of re-occlusion.
Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. A majority of patients with MAT have longstanding pulmonary disease. Rather than antiarrhythmic medication — optimizing pulmonary function is the best treatment approach. To our knowledge, the patient did well.
On his physical examination, cardiac and pulmonary auscultation was completely normal. Bi-phasic scan showed no dissection or pulmonary embolism. The lesion was successfully stented. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. He has 40 packs-year of smoking history. Turk Kardiyol Dern Ars.
Bedside ultrasound showed no effusion and moderately decreased LV function, with B-lines of pulmonary edema. Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? This was stented. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
His initial high sensitivity troponin I returned at 1300 ng/L and given that his cardiac workup was otherwise unremarkable, a CT was obtained to evaluate for pulmonary embolism and aortic aneurysm or dissection but this too was unrevealing. Also: electrical instability, pulmonary edema, or hypotension. Another EKG was also obtained.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". No pulmonary embolism is identified. First obtuse marginal also had an 80% stenosis and was stented. Pt received 324 ASA and 2 sprays of nitro with improvement. Cath lab was activated by EMS and transported emergent."
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content