This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The study, called IVUS-DCB, is the first randomized controlled trial to demonstrate the clinical benefits of using IVUS in angioplasty procedures for peripheral artery disease (PAD), a condition in which plaque builds up in arteries in the legs.
a leader in non-invasive artificial intelligence (AI) heart care solutions, introduced the next generation HeartFlow Plaque Analysis with an interactive experience. Having access to a patient’s whole coronary picture, with both quantified plaque and physiology, is a game changer as a clinician. F.A.C.C.
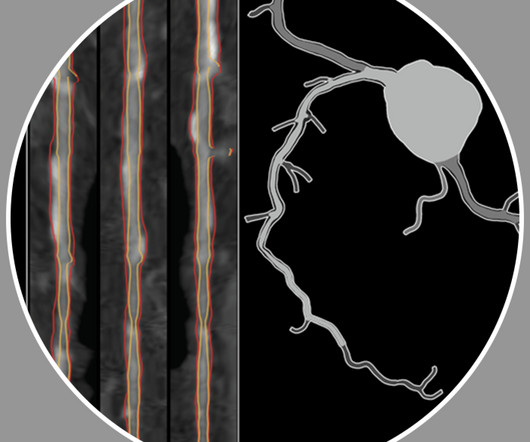
Objective The occurrence of ischemic stroke (IS) is closely related to the characteristics of carotid plaque (CP). Qualitative B-mode and CEUS features of carotid plaques were analyzed using a univariable and multivariable logistic regression to construct the CP score.
Coronary Intravascular Ultrasound (IVUS) equipment consists of an IVUS catheter, pullback device and the imaging console. IVUS Measurements Measurements include the measurement of lumen, plaque, calcium, remodeling, stent length and volumetric measurements. A vulnerable plaque and a plaque with ulceration or rupture can also be found.
Background To investigate the correlation between lg (circSCMH1/miR-874) and acute coronary syndrome (ACS), acute myocardial infarction (AMI), and carotid plaque stability. Compared with the low-risk plaque and control groups, the lg (circSCMH1/miR-874) value of medium-high risk plaque group decreased ( P < 0.05).
Bedside cardiac ultrasound with no obvious wall motion abnormalities. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. He was started on nitro gtt.
BackgroundPlaque progression (PP) is critical between subclinical atherosclerosis and plaque rupture. Journal of the American Heart Association, Ahead of Print. Small dense lowdensity lipoprotein cholesterol (sdLDLC) is considered as the most atherogenic lipoprotein.
You cannot eliminate the plaque entirely, but multiple clinical trials have shown plaque regression using high-intensity cholesterol-lowering treatments, which I have discussed previously. All of these parameters are important and need to be considered when evaluating plaque regression. REVERSAL Investigators.
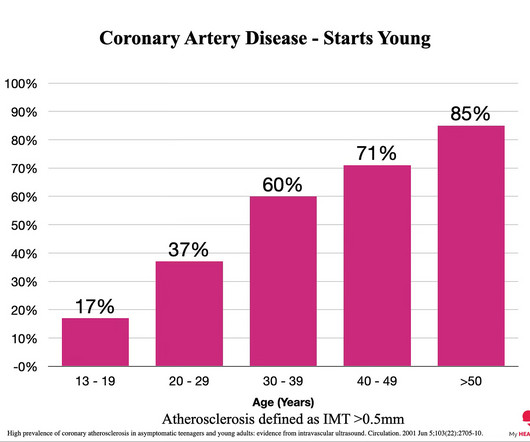
Everyone starts with no plaque in the coronary arteries, but over a long enough time frame, everyone develops plaque in their coronary arteries. By age 80, almost everyone will have evidence of advanced plaque in their coronary arteries, as defined by a cardiac CT 1. Plaque accumulation happens in stages. You got it.
We used carotid ultrasounds to detect plaque at baseline and follow‐up in 2006 to 2009 (median follow‐up=5.5 had incident plaque (109/1104 plaque‐free participants with baseline and follow‐up ultrasounds), 11.0% Lipids were measured after a 12‐hour fast. Approximately 2.8% During follow‐up, 9.9%
We report a case of TRAD in the early postoperative period, which was successfully managed with intravascular ultrasound-assisted endovascular intervention.Case presentationA 38-year-old man underwent HLA-compatible living kidney transplantation. Most cases are managed by operative repair.
Introduction:Nonstenotic carotid plaque is found in some patients with otherwise cryptogenic stroke (CS) but also in normal individuals and patients with stroke of known cause (KS). Methods of vessel imaging were carotid duplex ultrasound, CTA, and MRA. Stroke, Volume 56, Issue Suppl_1 , Page ATP296-ATP296, February 1, 2025.
Introduction Intravascular ultrasound (IVUS) improves clinical outcome in patients undergoing percutaneous coronary intervention (PCI) but dedicated prospective studies assessing the safety and efficacy of IVUS guidance during primary PCI are lacking.
The incidence of no-reflow was higher in patients with attenuated plaque ≥5 mm in length as evaluated by intravascular ultrasound (IVUS).Objective:The The proportion of low attenuation plaque observed by IVUS with a length of ≥5 mm was significantly higher in the no-reflow group compared to the reflow group (52.6%
BACKGROUND:HIV and hepatitis C virus (HCV) are associated with increased risk of carotid artery atherosclerotic plaque and stroke. Plaques were characterized from 6 areas of the right carotid artery. 2.78]) were each associated with higher prevalence of predominantly echogenic plaque. Stroke, Ahead of Print.
Carotid ultrasound results were divided into two groups based on the presence or absence of plaque. Carotid plaque was observed in 1140 (43.5%) subjects and CACS>0 in 1172 (44.7%) subjects. Lp(a) levels were categorized into two groups: below 50 mg/dl and 50 mg/dl or higher. 1692 (64.6%) were male.
Incident carotid plaques and their vulnerability were detected by carotid ultrasound at follow-up (2021). Higher sdLDL-C or sdLDL-C/LDL-C ratio, but not LDL-C, was significantly associated with an increased risk of incident carotid plaques. years (SD=0.14). years (SD=0.14). 9.90];P=0.027;Pfor linear trend=0.025).
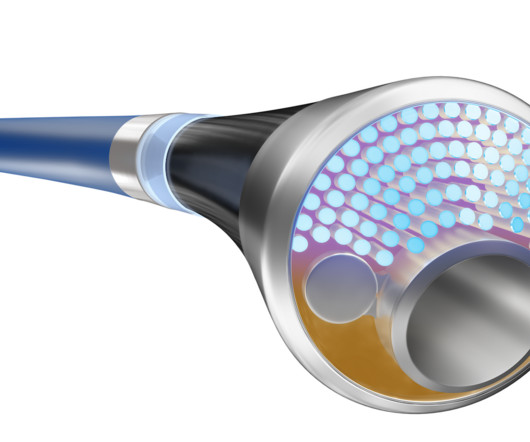
The Philips laser catheter integrates two critical PAD treatments into a single device, significantly simplifying the treatment workflow – atherectomy to remove atherosclerotic plaque from the internal surface of an artery, and intravascular lithotripsy to modify calcium deposits within the artery or disrupt calcium deposits in the artery wall.
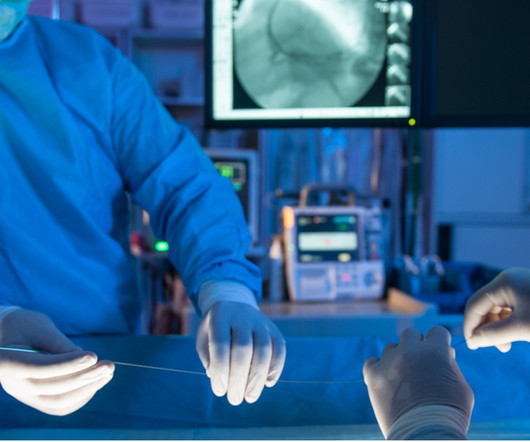
It provides detailed information about the vessel wall, plaque composition, and blood flow characteristics, enabling more accurate diagnosis and treatment planning. IVUS is a minimally invasive imaging technique that allows physicians to visualize the inside of blood vessels in real-time.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. Thus, intracoronary imaging modalities are crucial in this setting. From Gue at al.
In the subsample of patients without clinical CAD but with femoral plaque on ultrasound (n=58) who underwent cardiac computed tomography, 46% (n=27) had nonobstructive CAD and 28% (n=16) had obstructive CAD. The prevalence of CAD was 25.2% (n=97) (nonobstructive, 9.6% [n=37]; and obstructive, 15.6% [n=60]).
The primary outcome was the prevalence of carotid artery plaques assessed by ultrasound. Secondary outcomes included changes in NMR-derived lipoprotein subclasses and their mediation effects on carotid plaque. Fish oil supplementation was significantly associated with reduced prevalence of carotid plaques (P=0.023).
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. It is not rare.
Although it is statistically unlikely, multiple plaque ruptures are possible. On intravascular ultrasound (IVUS), the mid RCA plaque was described as "cratered, inflamed, and bulky," and the OM plaque was described as "bulky with evidence of inflammation and probably ulceration." Heitner et al.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing?
This in turn can enhance the chance of plaque build-up in the blood vessels of the heart (coronary arteries). Ultrasound image of the heart – echocardiogram, showing fluid collection around the heart, marked as PE, short for pericardial effusion. Reduced function of the thyroid gland is also associated with heart disease.
Smith comment : a very high proportion of MINOCA are ruptured plaque with lysed thrombus. That plaque is at risk of thrombosing again. It is worthwhile remembering that the majority of plaques which rupture are non-obstructive before they ulcerate and thrombose. Most plaque is outside the lumen!!
Invasive coronary imaging with intravascular ultrasound or optical coherence tomography should be used, when available, during index angiography to detect plaque disruption or spontaneous coronary artery dissection.
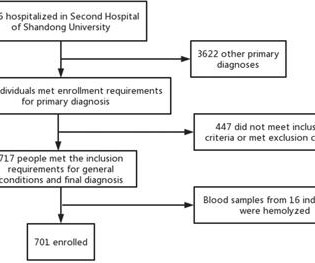
Residents aged 18 years or older in the sampled areas were included in this study, and data were collected through questionnaires, physical examinations, laboratory tests, carotid ultrasound examinations, and biological sample collection. A consent information platform for data collection and quality control management was also developed.
Plaque regression can be demonstrated by ultrasound evaluation of the carotids which are easily accessible. Of course, exercise burns out extra calories and reduces body weight, which in turn is due to a decrease in the fat deposits. Regular exercise can bring down the blood pressure in the long run.
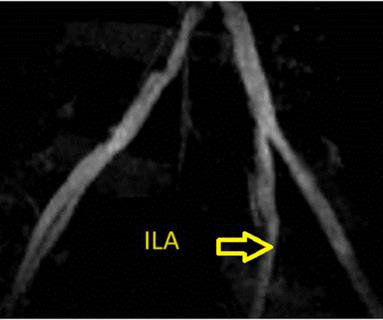
The left system showed no disease in the left main stem, but mild plaque disease in the dominant left circumflex artery. Intravascular ultrasound was also performed ( figure 1B ). The right coronary artery was small and free of disease. Angiographic findings of the left anterior descending artery are shown in figure 1A.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!!
As technologies advance and methodologies evolve, two crucial tools stand out for their pivotal roles in enhancing accuracy and efficacy: Optical Coherence Tomography (OCT) and Intravascular Ultrasound (IVUS). OCT employs light waves to capture high-resolution images, providing intricate details of vessel structures and plaque composition.
Bedside ultrasound with no apparent wall motion abnormalities, no pericardial effusion, no right heart strain. Angiography : --Culprit for the patient's unstable angina/Wellen syndrome is a ruptured plaque in the mid LAD. --As Course : Aspirin 325mg, chemistry, CBC, troponin panel all ordered.
In the rapidly changing field of cardiology, IVUS (Intravascular Ultrasound) and OCT (Optical Coherence Tomography) have seen significant growth. IVUS reveals plaque characteristics, optimal stent usage, and vessel measurements. Keeping up with the times isn't a choice anymore – it's a must.
We did a bedside cardiac ultrasound. The ECG and ultrasound could not have been differentiated from acute plaque rupture with occlusion of the RCA. So this ECG gets 8 points PLUS has excessive discordance in V1 PLUS has the finding in many leads, not just one. 3 points gets you an MI by Sgarbossa.
If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus." They often cannot even be recognized as culprits, as fissured or ulcerated plaque. What is Type 2 MI?
ET Main Tent (Hall B1) Coronary Sinus Reducer for the Treatment of Refractory Angina: A Randomised, Placebo-controlled Trial (ORBITA-COSMIC) Transcatheter Aortic Valve Implantation Versus Surgical Aortic Valve Replacement in Patients at Low to Intermediate Risk: One Year Outcomes of the Randomized DEDICATE-DZHK6 Trial Effect of Alcohol-mediated Renal (..)
Once stabilized, intravascular ultrasound showed significant thrombus and plaque in the LAD. Due to ongoing shock despite initial mechanical support, the patient was escalated to an Impella CP device after a transthoracic echo confirmed no left ventricle thrombus.
As technologies advance and methodologies evolve, two crucial tools stand out for their pivotal roles in enhancing accuracy and efficacy: Optical Coherence Tomography (OCT) and Intravascular Ultrasound (IVUS). OCT employs light waves to capture high-resolution images, providing intricate details of vessel structures and plaque composition.
Echocardiography – We can use ultrasound to visualize the heart and look at how well it pumps. With time, fat and cholesterol can get trapped in the areas of wear and tear and cause plaque formation. The plaques can damage us in 2 ways. This is termed as diastolic dysfunction.
On arrival, lung ultrasound confirmed pulmonary edema (B lines). Mild Plaque no angiographically significant obstructive coronary artery disease. There is STE and hyperacute T-waves in V2 and V3, with significant STE in I and aVL, and inferior reciprocal STD. This is proximal LAD Occlusion until proven otherwise.
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow). Now another, with ultrasound. What is the Diagnosis?
She had some very minor plaque but certainly nothing that could explain the heart attack and therefore she was discharged with a diagnosis of MINOCA i.e Then I think it is important that patient has an assessment of the function of the heart by means of an ultrasound to look for cardiomyopathies, Takotsubo etc.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content