This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
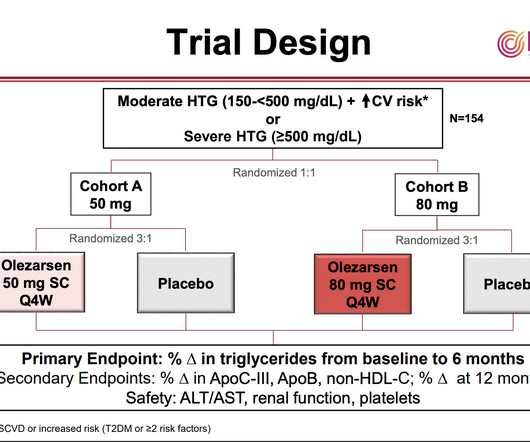
As with elevated LDL-cholesterol, high levels of triglycerides and the lipid particles on which they are carried in the blood can contribute to the formation of “plaques” in the arteries that impede blood flow and can lead to heart attacks and strokes. Triglycerides store unused calories and provide energy to the body.
A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. Angiography : --Culprit for the patient's unstable angina/Wellen syndrome is a ruptured plaque in the mid LAD. --As Am Heart J. 2000;139:430–436.
She was diagnosed with NSTEMI with a thrombolysis in myocardial infarction (TIMI) score of 5. Her EKG showed marked left-axis deviation, ST depressions in V2-V4, and RBBB. PCI, particularly with the Carlino technique, offers a reliable approach.
It is generally believed it is more of a mechanical plaque lesion. RCA and LCX Wellens do occur, making this entity’s perceived unique importance less certain 3. How common is thrombosis in the culprit artery of Wellen syndrome ? However by no means, we can say thrombosis do not occur. Is there a benign face of Wellen syndrome ?
Reperfusion of OMI indicates at least partial thrombolysis of occluding thrombus, but still unstable plaque rupture, which can reocclude at any moment. This case's first EMS ECG shows a rare example of LVH with active anterior and high lateral OMI. Comparison to prior ECG can be very helpful.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content