This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
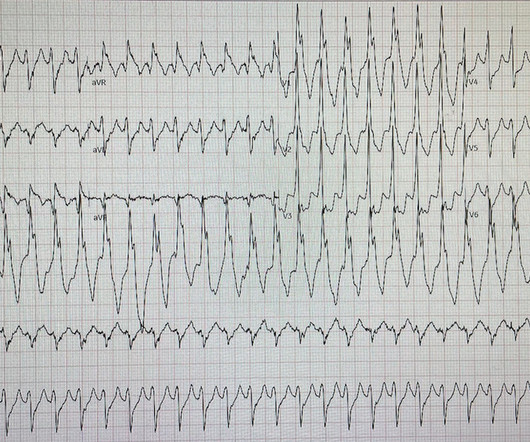
Ambulatory electrocardiography (ECG) monitoring revealed recurrent polymorphic ventricular tachycardia (PMVT). This case emphasises the importance of recognising plaque-associated CAS as a potential trigger for life-threatening arrhythmias, even in the absence of chest pain.
I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT. Of interest, he specified that he awoke earlier that morning in his usual state of health, then developed chest discomfort, then developed palpitations.
Here is her ED ECG: Here is the ED physician's interpretation: IMPRESSION UNCERTAIN REGULAR RHYTHM, wide complex tachycardia, likely p-waves. LEFT BUNDLE BRANCH BLOCK [120+ ms QRS DURATION, 80+ ms Q/S IN V1/V2, 85+ ms R IN I/aVL/V5/V6] Comparison Summary: LBBB and tachycardia are new. This is clearly ventricular tachycardia.
Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates). The underlying etiology is either Type 1 or Type II ischemia, although sometimes there’s overlap of both. Type I ischemia. Type II ischemia.
Learning Points: Type 1 MI is the type we are most familiar with: rupture of atherosclerotic plaque with production thrombus or platelet fibrin aggregates. You also appreciate the overly upright T waves in I and aVL which are reciprocal to the inferior T waves. But not all OMI is atherosclerotic in nature.
From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. McLaren : We’ve answered the first question – Sinus Tachycardia with episodic runs of wide QRS (RBBB morphology) and PVC’s.
Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. elevated BP), but rather directly correlated with coronary obstruction (due to plaque rupture and thrombosis) and, potentially, stymied TIMI flow. This results in Type I MI.
Conventional algorithm interpretation: SINUS TACHYCARDIA ABNORMAL RHYTHM ECG Confirmed by over-reading physician Transformed ECG by PM Cardio: PM Cardio interpretation: OMI with Low Confidence Dr. Rob Reardon did a bedside echo using Speckle tracking. Mild Plaque no angiographically significant obstructive coronary artery disease.
During active chest pain an ECG was recorded: Meyers ECG interpretation: Sinus tachycardia, normal QRS complex, STD in V2-V6, I, II, III and aVF. Subendocardial Ischemia from another Cause ( ie, sustained tachycardia — sinus or from some other arrhythmia; shock/profound hypotension; GI bleeding; anemia; etc. ).
Ramus: There is a large caliber branching ramus intermediate LAD is a medium caliber vessel that extends to the apex and is noted to have diffuse mild to moderate plaque in the midsegment. Post Procedure TIMI III. D1 is a medium caliber vessel, distal diagonal branches are small in caliber Echocardiogram Normal LV cavity size and thickness.
Systematic Assessment of the ECG in Figure-1: My Descriptive Analysis of ECG findings in Figure-1 is as follows: Sinus tachycardia at ~110/minute. A slightly prolonged QTc ( although this is difficult to assess given the tachycardia ). A normal PR interval. No chamber enlargement.
LAD plaque with 0-25 percent stenosis. That said, against acute PE — is the inconstancy of this patient's symptoms — the lack of tachycardia — and the lack of any other ECG signs of acute RV strain. Now, with elevated troponins, Wellens' syndrome is likely. A CT Coronary angiogram was ordered. CAD-RADS category 1. --No
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. 2) Tachycardia to this degree can cause ST segment changes in several ways. Sometimes you must correct the rhythm to see what lies underneath. Is this inferor STEMI?
There are multiple possible clinical situations that could account for diffuse subendocardial ischemia that is not due to ACS and plaque rupture. The history in today's case with sudden loss of consciousness followed by chest pain is very suggestive of ACS and type I ischemia as the cause of the ECG changes.
We can see enough to make out that the rhythm is sinus tachycardia. Tachycardia is unusual for OMI, unless the patient is in cardiogenic shock (or getting close). A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW.
A fast heartbeat is called tachycardia, while a slow heartbeat is called bradycardia in medical terms. Coronary artery disease Excessive cholesterol builds up plaque that blocks the arteries supplying blood to the heart. Arrhythmia In simple words, arrhythmia refers to an irregular heartbeat.
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow).
Although the shock is no doubt partly a result of poor pump function, with low stroke volume, especially of the RV, it should be compensated for by tachycardia. Cardiac output is stroke volume x rate, so this patient needs a higher heart rate. This is a perfect indication for atropine. He was successfully stented.
This was ruptured plaque with thrombus. The Initial ECG in Case #1: The ECG in Figure-1 shows sinus tachycardia at ~110/minute with markedly increased QRS amplitude and marked chest lead ST elevation. We have often made the point in Dr. Smith's ECG Blog that in general it is not common to see tachycardia with an uncomplicated MI.
One big chunk of ACS-UA is secondary UA where there is increased demand as in stable angina with tachycardia*. In these patients there is no plaque triggered ACS. For example, in a febrile patient who has associated HT, anemia, etc.,
This ECG was recorded: It is difficult to appreciate P-waves, but I believe this is sinus tachycardia. This was attributed to a "Type 2 MI", which is acute MI that is not due to ruptured plaque, but rather due to "supply demand oxygen mismatch". Bedside POCUS showed very poor LV function and a few pulmonary B lines.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). There were no plaques or stenoses. This patient very likely has some form of idiopathic ventricular tachycardia. Of the ventricular outflow tract tachycardias (RVOT-VT) makes up 80-90%.
In my review of the literature, there are many articles which purport to demonstrate an acutely increased risk of plaque rupture from emotional stress, but I could not find any credible case reports that were not at least as likely to be takotsubo. Mechanisms of plaque formation and rupture. Coronary plaque disruption.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content