This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
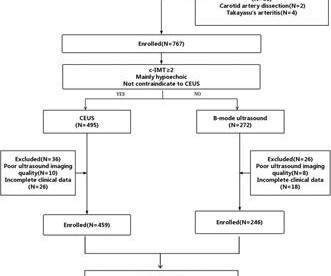
Objective The occurrence of ischemic stroke (IS) is closely related to the characteristics of carotid plaque (CP). Materials and methods This retrospective study evaluated 705 patients with low and intermediate carotid stenosis who underwent B-mode and CEUS from November 2021 to April 2023.
Bedside cardiac ultrasound with no obvious wall motion abnormalities. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. He was started on nitro gtt.
Coronary Intravascular Ultrasound (IVUS) equipment consists of an IVUS catheter, pullback device and the imaging console. IVUS Measurements Measurements include the measurement of lumen, plaque, calcium, remodeling, stent length and volumetric measurements. A vulnerable plaque and a plaque with ulceration or rupture can also be found.
We report a case of TRAD in the early postoperative period, which was successfully managed with intravascular ultrasound-assisted endovascular intervention.Case presentationA 38-year-old man underwent HLA-compatible living kidney transplantation. Most cases are managed by operative repair.
The Philips laser catheter integrates two critical PAD treatments into a single device, significantly simplifying the treatment workflow – atherectomy to remove atherosclerotic plaque from the internal surface of an artery, and intravascular lithotripsy to modify calcium deposits within the artery or disrupt calcium deposits in the artery wall.
Introduction:Nonstenotic carotid plaque is found in some patients with otherwise cryptogenic stroke (CS) but also in normal individuals and patients with stroke of known cause (KS). Methods of vessel imaging were carotid duplex ultrasound, CTA, and MRA. Stroke, Volume 56, Issue Suppl_1 , Page ATP296-ATP296, February 1, 2025.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. There may be a chronic tight stenosis and a non-obstructed lesion that thrombosed.
Incident carotid plaques and their vulnerability were detected by carotid ultrasound at follow-up (2021). Higher sdLDL-C or sdLDL-C/LDL-C ratio, but not LDL-C, was significantly associated with an increased risk of incident carotid plaques. years (SD=0.14). years (SD=0.14). 9.90];P=0.027;Pfor linear trend=0.025).
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing?
Bedside ultrasound with no apparent wall motion abnormalities, no pericardial effusion, no right heart strain. Angiography : --Culprit for the patient's unstable angina/Wellen syndrome is a ruptured plaque in the mid LAD. --As Course : Aspirin 325mg, chemistry, CBC, troponin panel all ordered.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Smith's comments in the May 19, 2020 post : — Non-obstructive coronary disease does not ne cessarily imply no plaque rupture with thrombus. It is not rare.
The LAD has diffuse disease with a few areas of moderate stenosis but no flow-limiting lesions. Although it is statistically unlikely, multiple plaque ruptures are possible. The PDA plaque was also bulky, but was not described as inflamed or ulcerated. The distal LCx is seen, and the OM is not well visualized here.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!!
The cardiologist called this 20% stenosis. Smith comment : a very high proportion of MINOCA are ruptured plaque with lysed thrombus. That plaque is at risk of thrombosing again. It is worthwhile remembering that the majority of plaques which rupture are non-obstructive before they ulcerate and thrombose.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus." They often cannot even be recognized as culprits, as fissured or ulcerated plaque. myocarditis).
History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. 2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.” Left main? 3-vessel disease?
Here are a couple shots with strain, or "speckle tracking" on ED Echo: To, me these look like anterior wall motion abnormality, but I showed them to one of our ultrasound fellows who is very interested in this. They read it as normal. She said: This is a tough one. Regional wall motion abnormality-distal septum and apex. It was stented.
Case Continued Bedside ultrasound was performed: This shows an anterior wall motion abnormality, and highly suggests the LAD as the infarct artery. Angiogram Culprit Lesion: 90% mid LAD stenosis with evidence of plaque rupture, TIMI III flow on angiography.
To, me these look like anterior wall motion abnormality, but I showed them to one of our ultrasound fellows who is very interested in this. She was treated medically for NonSTEMI, pending next day cath, which showed ulcerated plaque and a 60% thrombotic stenosis in the LAD distal to the first diagonal. It was stented.
Residents aged 18 years or older in the sampled areas were included in this study, and data were collected through questionnaires, physical examinations, laboratory tests, carotid ultrasound examinations, and biological sample collection. A consent information platform for data collection and quality control management was also developed.
A bedside ultrasound should be done to assess volume and other etiologies of tachycardia, but if no cause of type 2 MI is found, the cath lab should be activated NOW. In addition, the top left blue arrow indicates a section in the LAD with a severe stenosis, likely the culprit for the prior L A D occlusion which has since recanalized.
They did not have an ultrasound on the ambulance (some local crews are starting to utilize POC limited US in our service areas). He was taken to the cath lab and underwent emergent intervention: Thrombotic stenosis of the proximal RCA (95% with evidence of plaque rupture) is the culprit for the patient's inferoposterior STEMI.
The clinical presentation of ischaemic heart disease has a broad spectrum, encompassing not only traditional epicardial coronary artery disease (CAD) characterised by stenosis or occlusion but also structural and functional disorders at both macrovessel and microvessel levels, as highlighted in the latest European guidelines.
Provocative testing is very helpful for this Coronary Thrombus with lysis (one must do optical coherence tomography or at least intravascular ultrasound to find thes non-obstructive plaques that ruptured. These plaques will often not be recognized as "culprits", because no fissuring or ulcertaion is seen. Embolism with lysis.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content