This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
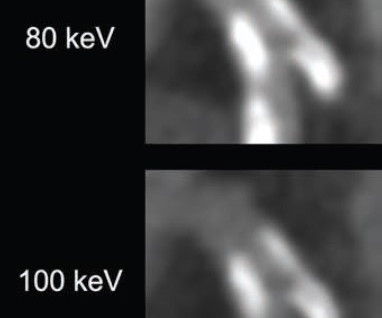
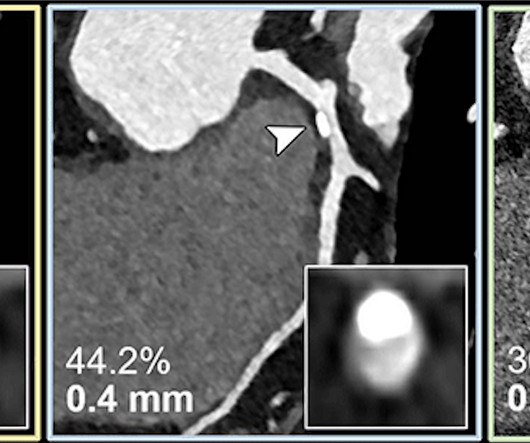
82-year-old man with calcified stenosis in left main artery who underwent coronary CTA by PCD CT. Curved multiplanar reformatted images at varying virtual monoenergetic imaging (VMI) levels (40-140 keV) show stenosis at each level. Percent diameter stenosis (PDS) decreased from 92.5% at 40 keV to 53.1% at 140 keV. at 140 keV.
The goal of the PREVENT trial was to compare the safety and efficacy of medical therapy along with focal preventive PCI of non-flow-limiting vulnerable plaque compared with medical therapy alone.
Coronary angiography identified moderate stenosis of the right coronary artery (RCA), without significant flow restriction by invasive pressure wire interrogation. This case emphasises the importance of recognising plaque-associated CAS as a potential trigger for life-threatening arrhythmias, even in the absence of chest pain.
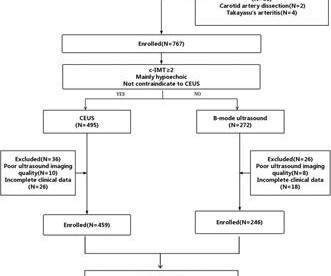
Objective The occurrence of ischemic stroke (IS) is closely related to the characteristics of carotid plaque (CP). Materials and methods This retrospective study evaluated 705 patients with low and intermediate carotid stenosis who underwent B-mode and CEUS from November 2021 to April 2023.
BackgroundThe utility of screening for the degree of common carotid artery (CCA) stenosis as a predictor of cardiovascular disease (CVD) in a general population remains unclear.Methods and ResultsWe studied 4775 Japanese men and women whose CCA was measured using bilateral carotid ultrasonography at baseline (April 1994–August 2001).
Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The pathologist may see a plaque that constitutes, for example, 50% of the cross-sectional area.
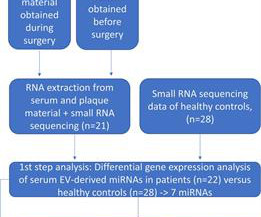
The early detection of plaques by circulating biomarkers is highly clinically relevant to prevent the occurrence of major complications such as stroke or heart attacks. miRNA expression profiles of serum-derived EVs were obtained by small RNA sequencing and in plaque material simultaneously acquired from patients.
mm (green outline) section thickness show the respective calcified plaque (arrowheads) and coronary stenosis (inset images). The reduced section thickness leads to less calcium blooming and therefore a less severe assessment of percentage of coronary stenosis in this patient. Curved multiplanar reconstructions with 0.6-mm
These key takeaways from the research letter on IVL-facilitated valvuloplasty for severely calcified mitral valve stenosis are published in the Journal of the American College of Cardiology (JACC) Cardiovascular Interventions. We are looking forward to treating patients who have no other options for mitral stenosis diseased valves.”
Background Although atherosclerosis (AS) can affect multiple vascular beds, previous studies have focused on the analysis of single-site AS plaques. The plaques were then categorized into culprit plaques, non-culprit plaques, and non-event plaques.
BackgroundIntracranial atherosclerotic stenosis is a leading cause of ischemic stroke and recurrent events due to plaque instability. Highresolution magnetic resonance imaging identifies plaque enhancement as a key marker of instability. After therapy, stenosis decreased from 75.9% (interquartile range, 69.5%84.8%)
BUT — Cardiac catheterization done a little later did not reveal any significant stenosis. Despite the absence of significant coronary stenosis on her post-arrest cath — the ECG in Figure-1 is clearly diagnostic of an extensive anterolateral STEMI ( presumably from acute LAD [ L eft A nterior D escending ] coronary artery occlusion).
BackgroundPlaque enhancement after gadolinium contrast administration may assess plaque instability and response to medical therapy. Plaque burden, degree of stenosis, and area degree of stenosis were calculated at baseline and follow‐up. Stroke: Vascular and Interventional Neurology, Volume 3, Issue 6 , November 1, 2023.
Background:Assessing carotid artery plaques in stenosis is crucial for treatment strategies and safety. This study explores the correlation between APT imaging and histopathological findings of carotid artery plaques in 34 consecutive patients who had carotid endarterectomy. E-04) and Group B (APT signal values < 1.90
Ipsilateral and contralateral carotid artery plaque features were compared, then the carotid artery plaque characteristics on the infarct side were correlated with the infarct pattern.Results:the mean age of subjects included was 68 years old, 79.6% of them were male. 0.15), larger wall area (0.50±0.19 0.23), all p values<0.05.
Background and Purpose:We aimed to investigate the effects of evolocumab, a proprotein convertase subtilisin/kexin type-9 inhibitor for intensive lipid-lowering, on intracranial atherosclerotic stenosis (ICAS).Methods:From The primary outcomes were the percentage change in plaque burden and plaque response (plaque regression >5%) rate.
Background:Previous research has suggested pericarotid fat density to be significantly linked to atherosclerotic plaque components and cerebrovascular events. Inflammatory markers within the plaques are critical in the pathogenesis and progression of carotid artery disease.
IntroductionHigh resolution vessel wall imaging (HR‐VWI) enables accurate visualization of intracranial atherosclerotic plaques. Radiomics can be utilized as an objective quantification method of plaque appearance and shape. Culprit plaques in the vascular territory of the stroke were identified.
Background:High-risk non-stenosing carotid plaque features are emerging as a possible source of embolism in the setting of ESUS. We utilized Fisher’s exact test to compare the frequencies of reporting each plaque characteristic.Results:We analyzed 152 CTA reports in depth.
Introduction:Nonstenotic carotid plaque is found in some patients with otherwise cryptogenic stroke (CS) but also in normal individuals and patients with stroke of known cause (KS). Overall, nonstenotic carotid stenosis ipsilateral to ischemic stroke was found in 33.5% (255/761) CS patients vs 19.2% (152/790) KS patients.
According to the writing group – co-led by SCCT Past President Koen Nieman , MD, PhD, MSCCT – well-described semi-quantitative scores and classifications are primarily based on visual interpretation or through categories of obstructive severity rather than exact percentage stenosis measurements.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. There may be a chronic tight stenosis and a non-obstructed lesion that thrombosed.
Asymptomatic high-grade carotid stenosis is an important therapeutic target for stroke prevention. Features like intraplaque hemorrhage on MRI and echolucency on B-mode ultrasonography can identify patients at higher risk of stroke with asymptomatic stenosis.
Introduction:A new Plaque-RADS classification (I-IV) is proposed to categorize the degree of carotid plaque instability and risk of embolic ischemic stroke. Carotid total plaque thickness and ulceration were scored by a neuroradiologist blinded to stroke side. N=188 plaques) met criteria. N=188 plaques) met criteria.
The bovine anatomical variation may alter the blood flow dynamics, potentially contributing to the formation and progression of carotid plaques. CTAs were reviewed to assess the carotid stenosis and the anatomy of the aortic arch. N=16, 36.4%; p=0.030). vs. 70.0% [50.0-95.0]; 95.0]; p=0.030)(Figure 3).Conclusions:The
Incident carotid plaques and their vulnerability were detected by carotid ultrasound at follow-up (2021). Higher sdLDL-C or sdLDL-C/LDL-C ratio, but not LDL-C, was significantly associated with an increased risk of incident carotid plaques. years (SD=0.14). years (SD=0.14). 9.90];P=0.027;Pfor linear trend=0.025).
The LM has an irregular 30% distal stenosis, followed by an 80% ostial LAD stenosis, and total occlusion of the LAD proximally with TIMI grade 1 flow in the distal vessel. The LCX demonstrates an ostial 80% stenosis prior to the bifurcation of a large OM artery. A large Diagonal artery has subtotal occlusion proximally.
The risk of stroke recurrence among patients with ICAD-related stroke is the highest among those with confirmed stroke and stenosis ≥70%. In fact, the 1-year recurrent stroke rate of >20% among those with stenosis >70% is one of the highest rates among common causes of stroke.
Materials and methods This retrospective, institutional-review board approved study included consecutive patients with calcified coronary artery plaques undergoing CCTA with PCD-CT and invasive coronary angiography between July and December 2022. Virtual monoenergetic images (VMI) and VNCa images were reconstructed. 68, ICC: 94 and 1%, p = .07,
Invasive plaque characterization of the SFA was performed by intravascular imaging using optical coherence tomography. Histological analysis of plaque specimens was performed after directional atherectomy. cm vs. 0.23 ± 0.11 cm; cm; 1.77 ± 0.19 vs. 1.57 ± 0.15; p -value <0.05). cm vs. 0.23 ± 0.11 cm; cm; 1.77 ± 0.19
The breakthrough designation, according to the Milpitas, CA-based technology company, is for an indication to improve coronary luminal diameter, restore hemodynamic modulation, and reduce plaque progression in patients with symptomatic ischemic heart disease due to discrete de novo native coronary artery lesions. of the U.S. population.
The Philips laser catheter integrates two critical PAD treatments into a single device, significantly simplifying the treatment workflow – atherectomy to remove atherosclerotic plaque from the internal surface of an artery, and intravascular lithotripsy to modify calcium deposits within the artery or disrupt calcium deposits in the artery wall.
3% sodium alginate solution was cast into a stenosis mold and crosslinked in a 40% calcium chloride. The deformable gel constituted an 8mm long replaceable stenotic segment at the level of M1‐MCA simulating an atherosclerotic plaque with a 0.5mm internal diameter. An initial stenosis flow rate was registered with a value of 8.5 ± 5.33
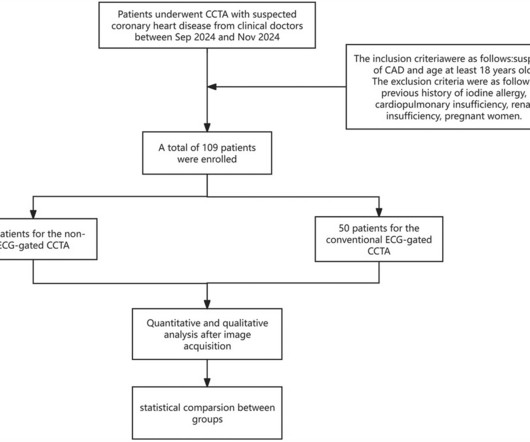
The application of AI technology in the diagnosis of cardiovascular diseases using coronary CT angiography (CCTA) has gradually deepened, and efficient and intelligent methods are optimizing and reshaping the clinical diagnosis pathways, including optimization of image quality, fully automated calculation of calcification score, coronary stenosis, (..)
A healthy young man would be expected to have a troponin that is undetectable (less than 3 ng/L) The patient went to the cath lab: --Ruptured plaque in the distal LAD --Diffuse coronary artery disease is noted in LAD branch vessels and a small LPL branch -- LAD is a large-caliber vessel that wraps around the apex (this explains the STE in inferior (..)
With Plaque Features Associated with False Positives. Coronary CTA With AI-QCT Interpretation: Comparison With Myocardial Perfusion Imaging for Detection of Obstructive Stenosis Using Invasive Angiography as Reference Standard. Presented at the European Association of Cardiovascular Imaging: Late Breaking Clinical Research and Trials.
IVUS Measurements Measurements include the measurement of lumen, plaque, calcium, remodeling, stent length and volumetric measurements. Plaque morphology assessment with IVUS Plaque morphology can be assessed in terms of its geometry and echogenicity. A vulnerable plaque and a plaque with ulceration or rupture can also be found.
Lp(a) is emerging as an important, yet under-recognized, potential risk factor for cardiovascular disease due to its ability to promote the development of plaques within artery walls, clot formation and aortic valve calcification. 2022 Aug, 80 (9) 934946 Kronenberg F.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Smith's comments in the May 19, 2020 post : — Non-obstructive coronary disease does not ne cessarily imply no plaque rupture with thrombus. It is not rare.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing?
Angiography : --Culprit for the patient's unstable angina/Wellen syndrome is a ruptured plaque in the mid LAD. --As Two ECG patterns were described by the original investigators in 1982 as being consistent with a Wellens’ Syndrome prediction of high-grade LAD stenosis.
Anaphylaxis leads to plaque rupture or erosion leading to acute myocardial infarction (type II) and acute coronary stent thrombosis (type III). Emergency coronary angiography showed coronary spasm and moderate lumen stenosis in the middle segment of left anterior descending artery (LAD).
Although carotid plaques can be identified on CT angiography (CTA), interpretation is challenging for frontline physicians. Quantification of plaque volume/composition requires much manual effort. For detection of calcific and hypodense plaque components, respectively, the model achieved sensitivity of 96.5% (95%CI:89.3-99.1%)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content