This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundPlaque progression (PP) is critical between subclinical atherosclerosis and plaque rupture. After multivariate adjustment, every 0.1mmol/L increase in timeaveraged sdLDLC conferred a 1.2fold increased risk of PP.ConclusionsOur findings suggest that sdLDLC is an independent riskfactor of PP in patients with coronary artery disease.
We used carotid ultrasounds to detect plaque at baseline and follow‐up in 2006 to 2009 (median follow‐up=5.5 had incident plaque (109/1104 plaque‐free participants with baseline and follow‐up ultrasounds), 11.0% Lipids were measured after a 12‐hour fast. Approximately 2.8% During follow‐up, 9.9%
We report a case of TRAD in the early postoperative period, which was successfully managed with intravascular ultrasound-assisted endovascular intervention.Case presentationA 38-year-old man underwent HLA-compatible living kidney transplantation. Most cases are managed by operative repair.
BACKGROUND:HIV and hepatitis C virus (HCV) are associated with increased risk of carotid artery atherosclerotic plaque and stroke. Plaques were characterized from 6 areas of the right carotid artery. 2.78]) were each associated with higher prevalence of predominantly echogenic plaque. Stroke, Ahead of Print.
Incident carotid plaques and their vulnerability were detected by carotid ultrasound at follow-up (2021). Higher sdLDL-C or sdLDL-C/LDL-C ratio, but not LDL-C, was significantly associated with an increased risk of incident carotid plaques. years (SD=0.14). years (SD=0.14). 9.90];P=0.027;Pfor linear trend=0.025).
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. Thus, intracoronary imaging modalities are crucial in this setting. From Gue at al.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing?
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. It is not rare.
ET Murphy Ballroom 4 Health 360x Registry: Scalable Workforce for Equitable Access to Point of Care Decentralized Clinical Trials Prevalence of Cardiovascular Disease and RiskFactors Among National Football League Alumni and Their Family Members: Results from the Huddle Study Hózhó (Heart Failure Optimization at Home to Improve Outcomes): A Pragmatic (..)
If the arrest was caused by acute MI due to plaque rupture, then the diagnosis is MINOCA. Here is my comment on MINOCA: "Non-obstructive coronary disease" does not necessarily imply "no plaque rupture with thrombus." They often cannot even be recognized as culprits, as fissured or ulcerated plaque. What is Type 2 MI?
She had some very minor plaque but certainly nothing that could explain the heart attack and therefore she was discharged with a diagnosis of MINOCA i.e Genetics and physiological stress are also riskfactors. She agreed and we performed an angiogram and we were fully expecting a blockage but interestingly there weren’t any.
A completely healthy 30-something year old woman with no cardiac riskfactors had sudden onset of bilateral trapezius pain that radiated around to her throat. R Riskfactors = 0 5. Risk of 30-day adverse events is less than 1.7%. She called 911. mm at the J-point, relative to the PQ junction. A Age: = 0 4.
A completely healthy 30-something year old woman with no cardiac riskfactors had sudden onset of bilateral trapezius pain that radiated around to her throat. R Riskfactors = 0 5. Risk of 30-day adverse events is less than 1.7%. The ECG told the story. The first troponin was below the level of detection (LoD).
At baseline visit, women will be randomized to undergo 2D/3D/strain vascular ultrasound (360 with imaging vs. 360 age- and RF-matched controls without imaging). Imaging can play a key role by revealing the presence of atherosclerotic plaques in a directly relatable way and thus, larger effects are anticipated in women with plaques.
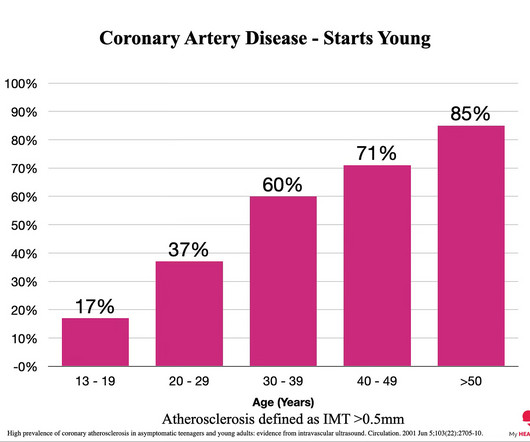
To understand why the answer is always ‘Now’, I want to highlight three key points and then point to the evidence that supports the idea that reducing risk early is always better. Everyone starts with no plaque in the coronary arteries, but over a long enough time frame, everyone develops plaque in their coronary arteries.
However, its value in patients with carotid plaque stability remains unclear. Carotid ultrasound was used to determine the stability of carotid plaque. Logistic regression was used to analyze the relationship between the TyG index and unstable carotid plaque.
CVD risk was assessed using QRISK3 (which includes SLE diagnosis as a riskfactor) and Framingham Risk Score. This atherosclerosis risk signature was validated in a second adult female SLE cohort (n=98) that predicted plaque status with moderate accuracy (area under the receiver operating characteristic curve, 0.79).
Recently, clonal hematopoiesis of indeterminate potential (CHIP) has emerged as a riskfactor for cardiovascular diseases. Assessment of carotid artery atherosclerosis was performed with ultrasound. Surprisingly, the presence of atherosclerotic plaques was significantly lower in individuals with CHDMs.
Smith Major Learning Point: The worst riskfactor for a bad outcome in OMI is young age because cardiologists cannot believe that a young person can have an OMI. Only after her troponin peaked at 500,000 ng/L did she get her angiogram, which showed a 100% left main occlusion due to ruptured plaque. This gets drilled into them.
Heart disease, the build-up of plaque in the coronary arteries, typically starts years, if not decades, prior to an event. In many cases, you can see the risk coming years in advance. This doesn't apply to everyone, but on average, you can see the risk coming. The more plaque, the higher the risk. Here’s why.
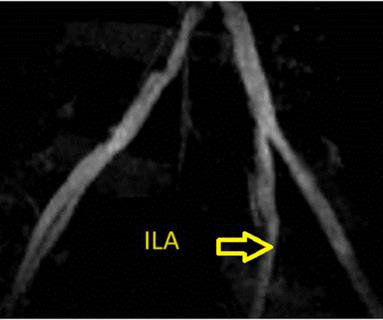
Provocative testing is very helpful for this Coronary Thrombus with lysis (one must do optical coherence tomography or at least intravascular ultrasound to find thes non-obstructive plaques that ruptured. These plaques will often not be recognized as "culprits", because no fissuring or ulcertaion is seen. Embolism with lysis.
In this case, the context is a 51 year old man with riskfactors presenting with acute onset substernal chest pain with nausea and vomiting. The operator performed intravascular ultrasound and visualized acute plaque rupture with thrombus formation and placed a stent. So an equivocal (or even normal) EKG is not enough.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content