This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
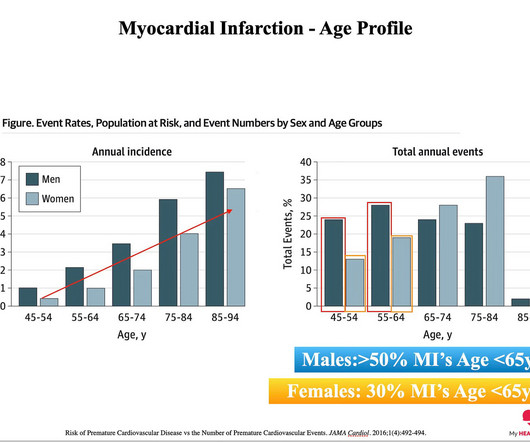
The reason: They were accumulating plaque in their coronary arteries much earlier than their peers. You can’t have a heart attack if you don’t have plaque in your coronary arteries. And plaque in your coronary arteries is the result of exposure to riskfactors over time. The answer: RiskFactors.
Plaque volumetric measurements showed that total plaque volume (1,103.50285.51mm3 vs. 913.18277.45mm3; p<0.001) and calcified plaque volume (149.77160.71mm3 vs. 36.4226.86mm3; p<0.001) were more pronounced in individuals in the significant CAD group than those in the non-significant CAD group. vs. 39.1668.88; p<0.001).
In this 6-month randomized controlled study, twice-weekly HIIT reduced coronary plaque volume, increased aerobic fitness, and improved body composition in adults with stable heart disease, suggesting benefits for cardiovascular disease progression. Does this greater plaque presence put athletes at a greater risk of CVD events?
Aging is known to be a riskfactor for the biological changes that create the dangerous buildup of plaque in arteries called atherosclerosis, and aging also induces a buildup of memory CD8 T cells, a type of immune cell, in mice and humans.
Metal exposure from environmental pollution is associated with increased buildup of calcium in the coronary arteries at a level that is comparable to traditional riskfactors like smoking and diabetes, according to a study by Columbia University Mailman School of Public Health.
This case report describes an atypical presentation of CAS in a 68-year-old white British male with cardiovascular riskfactors. This case emphasises the importance of recognising plaque-associated CAS as a potential trigger for life-threatening arrhythmias, even in the absence of chest pain.
Metal exposure from environmental pollution is associated with increased calcium buildup in the coronary arteries at a level comparable to traditional riskfactors, according to a new study.
Background Inflammation plays a pivotal role in atherogenesis and is a causal riskfactor for atherosclerotic cardiovascular disease. Non-invasive coronary CT angiography (CCTA) enables evaluation of coronary plaque phenotype. Baseline total plaque volume was 1394 (1036, 1993) mm 3. Results The mean±SD age was 65.4±8.4
Multiple studies have shown plaque build up in people from their teenage years onwards with significant amounts present by mid 20’s. This is why addressing riskfactors such as high cholesterol early in life is so important. I presume most of you who are reading this are well past your twenties.
BackgroundPlaque progression (PP) is critical between subclinical atherosclerosis and plaque rupture. After multivariate adjustment, every 0.1mmol/L increase in timeaveraged sdLDLC conferred a 1.2fold increased risk of PP.ConclusionsOur findings suggest that sdLDLC is an independent riskfactor of PP in patients with coronary artery disease.
The complex development of atherosclerosis manifests as intimal plaque which occurs in the presence or absence of traditional riskfactors. CCTA also has the potential to de-risk clinical endpoint-based trials both financially and by enrichment of participants at higher likelihood of MACE.
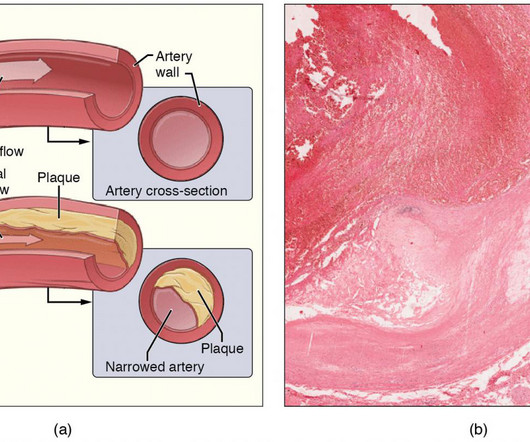
Inflammation and Plaque Buildup: Smoking damages the endothelium (the inner lining of blood vessels), triggering inflammation. This damage accelerates the formation of plaques, leading to atherosclerosisa condition where arteries narrow and harden, restricting blood flow.
Artery Damage : Hypertension damages the inner lining of your arteries, making them less elastic and more prone to plaque buildup. This condition, called atherosclerosis, narrows the arteries, restricting blood flow and increasing the risk of heart attacks and strokes.
Although the entire vascular bed is constantly exposed to the same riskfactors, atherosclerosis manifests a distinct intra-individual pattern in localization and progression within the arterial vascular bed.
Advancements in magnetic resonance angiography (MRA) with vessel wall imaging (VWI) have enabled the identification of vulnerable plaques, aiding in risk stratification for neurovascular events. A retrospective chart review was conducted to extract pertinent clinical data including cardiovascular riskfactors and medications.
BACKGROUND:HIV and hepatitis C virus (HCV) are associated with increased risk of carotid artery atherosclerotic plaque and stroke. Plaques were characterized from 6 areas of the right carotid artery. 2.78]) were each associated with higher prevalence of predominantly echogenic plaque. Stroke, Ahead of Print.
Lp(a) is emerging as an important, yet under-recognized, potential riskfactor for cardiovascular disease due to its ability to promote the development of plaques within artery walls, clot formation and aortic valve calcification. The development of the Tina-quant Lipoprotein (a) Gen.2
Incident carotid plaques and their vulnerability were detected by carotid ultrasound at follow-up (2021). Higher sdLDL-C or sdLDL-C/LDL-C ratio, but not LDL-C, was significantly associated with an increased risk of incident carotid plaques. years (SD=0.14). years (SD=0.14). 9.90];P=0.027;Pfor linear trend=0.025).
We used carotid ultrasounds to detect plaque at baseline and follow‐up in 2006 to 2009 (median follow‐up=5.5 had incident plaque (109/1104 plaque‐free participants with baseline and follow‐up ultrasounds), 11.0% We evaluated SHFS participants, who were 15 to 39 years old at the baseline examination in 2001 to 2003 (n=1440).
Atherosclerotic plaque formation is modulated by genetic and environmental interactions. In this study, we examined the effects of ApoE deficiency and high fat diet (HFD) on plaque formation and immunomodulatory cellular and molecular mechanisms in mice models.Methods:Wild type and ApoE knockout (KO) mice were fed with normal or HFD.
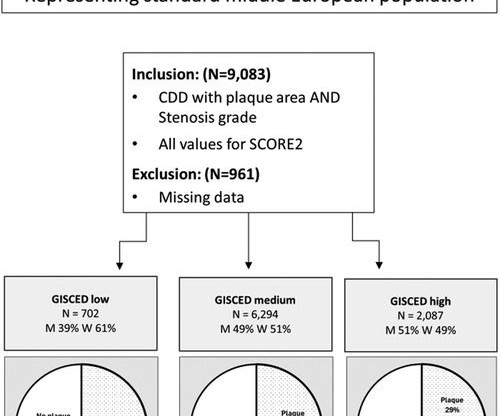
Nevertheless, most cardiovascular risk models, including SCORE2, still do not take educational status into account even if this factor is easily assessed and costs nothing to acquire. Even after adjusting for common riskfactors including metabolic syndrome and SCORE2, the relationship was maintained. 2.06; and 0.0.63
fold higher risk for cardiac mortality and 5.5-fold fold higher risk for major adverse cardiac events (MACE) Caristo's AI-Risk model, CaRi-Heart Risk Score, outperformed other scores in routine clinical use for prediction of cardiac mortality, and when presented to clinicians, resulted in changes of management decision in 45% of the patients.
The degree of CCA stenosis was associated with increased risks of incident CVD, coronary heart disease, and stroke, with multivariable‐adjusted HRs (95% CIs) for <25%, 25%–49%, and ≥50% stenosis with plaque compared with no CCA plaque of 1.37 (1.07–1.76), 1.76), 1.72 (1.23–2.40), 2.40), and 2.49 (1.69–3.67),
Carotid plaque (CP) is an independent riskfactor for cardiovascular diseases. However, evidence for association of MHR with risk of CP is scarce.Methods and ResultsThis study involved 5260 participants aged >18 years old from the Dalian health management cohort in 2014 to 2022.
Non-obstructive coronary disease at the time cardiac cath is done does not necessarily imply there was no plaque rupture with thrombus. These plaques will often not be recognized as "culprits" — because no fissuring or ulceration is seen. Longterm prognosis of patients with MINOCA clearly depends on the underlying etiology.
MINOCA may be due to: coronary spasm, coronary microvascular dysfunction, plaque disruption, spontaneous coronary thrombosis/emboli , and coronary dissection; myocardial disorders, including myocarditis, takotsubo cardiomyopathy, and other cardiomyopathies. Thus, intracoronary imaging modalities are crucial in this setting. From Gue at al.
Any atherosclerotic plaque is bad, and its presence portends a worse prognosis if modifiable riskfactors like hypertension and smoking are not addressed.
We investigated whether treatment with LDE-paclitaxel changes plaque progression by coronary CT angiography and is safe in patients with chronic coronary artery disease. Baseline demographics, riskfactors, and laboratory results were not different between groups.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. It is not rare.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). Smith comment : Is the ACS (rupture plaque) with occlusion that is now reperfusing?
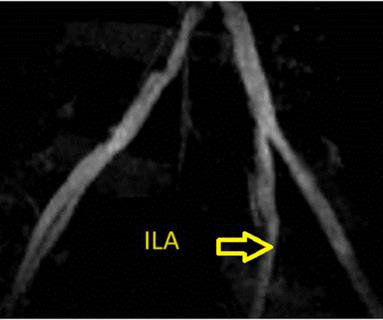
Angiography showed a donor renal artery dissection distal to the moderately stenosed anastomosis site with calcified atherosclerotic plaque confirmed by IVUS. Our case showed that endovascular intervention can replace surgery to repair very early vascular complications such as dissection and help patients avoid high-risk operations.
I quickly reviewed the patient’s records and saw that she was a 53 year old woman with a history of BMI 40, but no other identifiable riskfactors for coronary artery disease. Learning Points: Type 1 MI is the type we are most familiar with: rupture of atherosclerotic plaque with production thrombus or platelet fibrin aggregates.
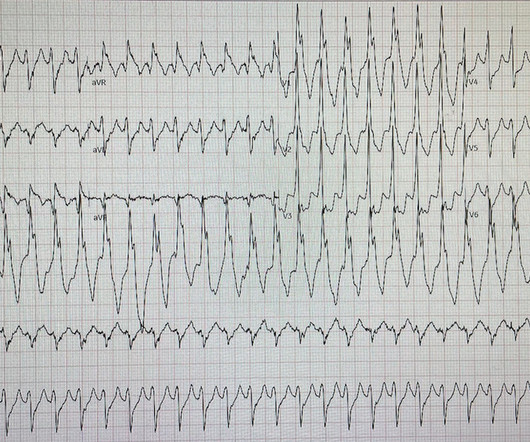
He denied any known history of CAD, but did report ASCVD riskfactors to include HTN, HLD, and DM. I interpreted the ECG as VT with two primary etiological possibilities: 1. Abrupt plaque ulceration of Type 1 ACS leading to VT.
The vessels with reduced CFR presented a significantly higher prevalence of obstructive CAD (37% vs. 26%; P < 0.001), diffused atherosclerosis (22% vs. 11%; P < 0.001), low-attenuation plaque (6% vs. 3%; P = 0.030), and positive remodeling (7% vs. 2%; P = 0.001). FAI was higher in vessels with reduced CFR (−80.8 HU HU vs. −81.8 HU;
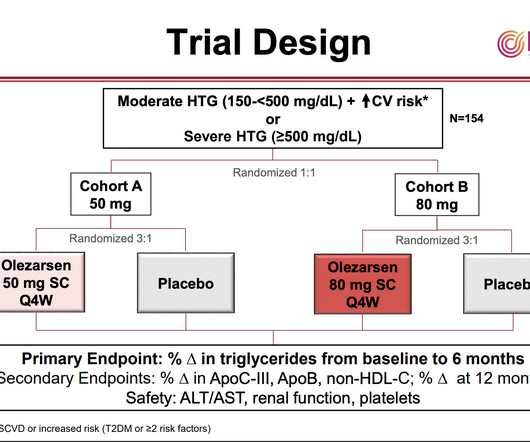
As with elevated LDL-cholesterol, high levels of triglycerides and the lipid particles on which they are carried in the blood can contribute to the formation of “plaques” in the arteries that impede blood flow and can lead to heart attacks and strokes. Triglycerides store unused calories and provide energy to the body. and Canada.
Immune-mediated inflammatory diseases (IMIDs) are recognised riskfactors for accelerated atherosclerotic cardiovascular disease (CVD), particularly in younger individuals and women who lack traditional CVD riskfactors.
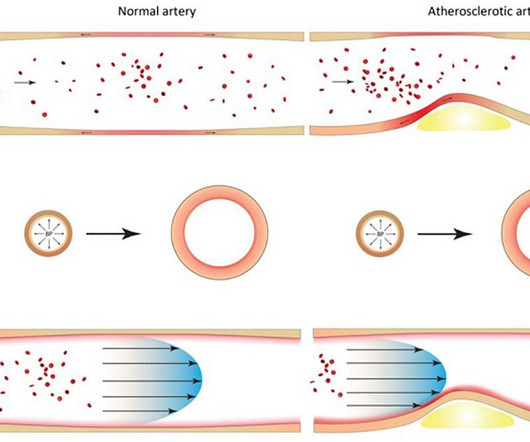
IntroductionAtherosclerosis, the hardening and narrowing of the arteries, occurs due to the buildup of plaque on the inner walls of the arteries which can result in reduced blood flow to the organs and tissues. Riskfactors such as smoking, chronic kidney disease, and aging can contribute to plaque formation.
Understanding the riskfactors, recognizing the signs and seeking guidance from a cardiologist can play a significant role in preventing and treating this disease. Identifying Those at Risk for Heart Disease Heart disease describes a range of disorders that affect the cardiovascular system and the heart.
M-MDSCs phenotype switch, atherosclerotic lesion development and plaque phenotype was studiedin vivo.Results:We observed CCR5 elevation on Monocytic-MDSCs in the early phase of atherosclerosis. MDSCs phenotype and functionality were assessed using CCR5 inhibitorin vitro(10-8M) andin vivo(i.p 3ng/day for 15 days).M-MDSCs
Lp(a) (lipoprotein [a]) has recently garnered attention as an independent riskfactor for astherosclerotic cardiovascular disease, with proinflammatory and prothrombotic mechanisms contributing to its atherogenicity. Atherosclerotic cardiovascular disease is a major health concern worldwide and requires effective preventive measures.
High-grade stenosis with poor collaterals can cause hemispheric hypoperfusion, and unstable plaque can cause microemboli, both of which may be treatable riskfactors for cognitive impairment. New riskfactors are emerging, like exposure to microplastics and nanoplastics.
High levels of triglycerides and the lipid particles on which they are carried in the blood can contribute to the formation of “plaques” in the arteries that impede blood flow and can lead to heart attacks and strokes. An estimated 1 in 5 U.S. Patients’ average triglyceride level at baseline was about 900 mg/dL.
Nevertheless, the relationship between CAC and the susceptibility of a plaque to provoke a thrombotic event remains incompletely understood. This review summarizes the current understanding and literature on CAC.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content