This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
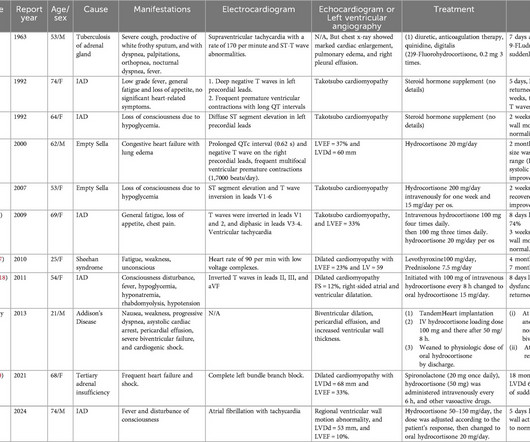
Cardiac ultrasound showed significantly reduced left ventricular ejection fraction (LVEF; 10%). Subsequently, the patient was initially administered intravenous injection of hydrocortisone (50150mg/day) for 5 days, and then transitioned to a physiological supplement dose orally. This indicated adrenal crisis.
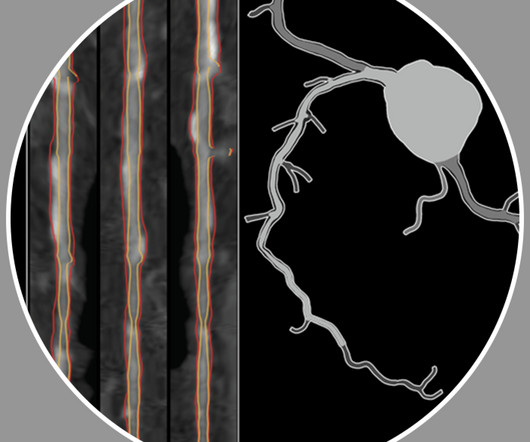
Having access to a patient’s whole coronary picture, with both quantified plaque and physiology, is a game changer as a clinician. Prospective Deep Learning-based Quantitative Assessment of Coronary Plaque by CT Angiography Compared with Intravascular Ultrasound EHJ 2024. medical director of CV imaging, nuclear and CT, Charleston, WV.
Here was his cardiac echo (remember, done 9 hours after the one above): Pericardial Effusion with Tamponade physiology, developed within 9 hours. Here was his echo that evening: Continued 9 hours later: the patient presented with fever and hypotension.
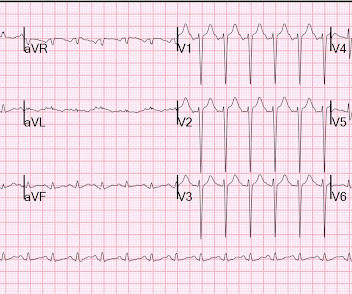
Gallbladder ultrasound was negative for stones. Respect physiology. The abrupt transition that we see in ECG #1 — from the very small, upright T wave in lead V2 — to the disproportionately larger ( taller than its R wave ) "bulky" ST-T wave in lead V3 — is simply not physiologic. Chest x-ray was normal.
This case was posted on the [link] ultrasound site, of which this ECG blog is a part. I refer you to the video case presentation by one of my colleagues, Dr. Rob Reardon (who has, by the way, a fantastic collection of ED ultrasound cases). However, only the first ECG was shown, and it was recorded before the patient became ill.
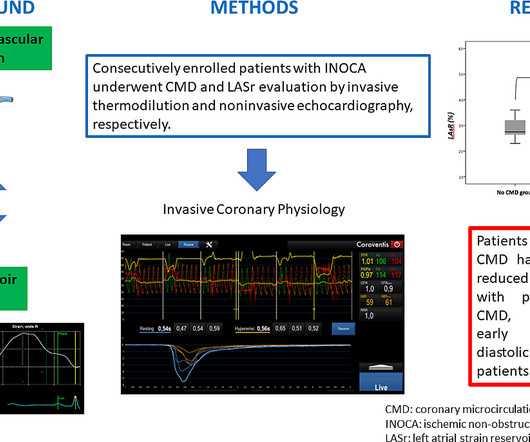
Coronary microvascular dysfunction (CMD) refers to structural and functional abnormalities of the coronary microcirculation, which may be diagnosed using invasive coronary physiology. CMD is responsible for im.
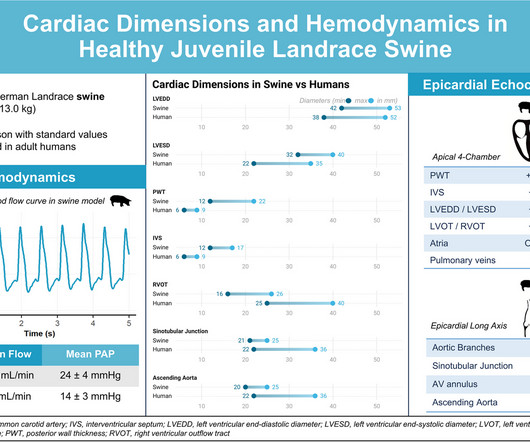
Swine are frequently used as animal model for cardiovascular research, especially in terms of representativity of human anatomy and physiology. Reference values for the most common species used in research are.
On intravascular ultrasound (IVUS), the mid RCA plaque was described as "cratered, inflamed, and bulky," and the OM plaque was described as "bulky with evidence of inflammation and probably ulceration." Additional findings: No ST elevation." From angiography, it is not clear what the culprit is. The basic facts are these: Morphine works.
Cardiac Ultrasound may be a surprisingly easy way to help make the diagnosis Answer: pulmonary embolism. Now another, with ultrasound. The ECG accurately reflects the physiologic state of the underlying myocardium, but there is always more than one possible etiology of that physiologic state. What is the Diagnosis?
For example, by integrating Ventripoint’s AI-powered heart-scanning technology, which turns ultrasound images of the heart into MRI-quality heart images, InView provides pediatric cardiologists with access to MRI-quality heart images at a fraction of the cost and time needed for traditional MRIs.
Given her risk factors (HTN, HLD, ESRD from diabetes) I decided to obtain a broad cardiac workup for the patient: serial ECGs, labs, serial troponins, CXR and bedside cardiac ultrasound. Ultrasounds can be very helpful in guiding your diagnostic pathway: location of WMA on US led to obtaining posterior leads.
Smith comment: This patient did not have a bedside ultrasound. Had one been done, it would have shown a feature that is apparent on this ultrasound (however, this patient's LV function would not be as good as in this clip): This is recorded with the LV on the right. In fact, bedside ultrasound might even find severe aortic stenosis.
This is an ultrasound (a bit like the type that we use on pregnant women to look at the baby). An ultrasound will allow you to visualise the heart, measure the sizes of the chambers, assess the heart valves and work out how well the heart functions as a pump. An echo is easy to do, risk free and easily accessible.
So I immediately left the room to get an ultrasound machine. While calling for some help and arranging to have her transported to our critical care zone, I got this quick ultrasound which confirmed my suspicion: This quick view was all I was able to obtain in the circumstances.
Genetics and physiological stress are also risk factors. Then I think it is important that patient has an assessment of the function of the heart by means of an ultrasound to look for cardiomyopathies, Takotsubo etc. myocarditis), and blood clotting disorders.
Case continued: All the physicians were very worried about LAD occlusion and recorded a couple bedside ultrasounds: This shows a profound apical and septal wall motion abnormality, perfectly consistent with LAD OMI. These ultrasounds confirm LAD occlusion. This T wave progression sequence does not make physiologic sense.
So we did a bedside cardiac ultrasound. PEARL #3: There is a physiologic reason why pulmonary hypertension from advanced RVH may result in a qR pattern in lead V1 ( Figure-2 ). I looked through her chart and found a formal echo from the last visit showing "Severe right ventricular enlargement and decreased RV systolic function".
They did not have an ultrasound on the ambulance (some local crews are starting to utilize POC limited US in our service areas). Case continued EMS immediately transported, activated the cath lab and gave 324 mg aspirin en route. It was about a 7 minute transport time.
Check : [vitals, SOB, Chest Pain, Ultrasound] If the patient has Abdominal Pain, Chest Pain, Dyspnea or Hypoxemia, Headache, Hypotension , then these should be considered the primary chief complaint (not syncope). Fourth, syncope in the elderly often results from polypharmacy and abnormal physiologic responses to daily events.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content