This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. The physiologic reason for this — is thought to be the result of momentarily increased circulation from mechanical contraction arising from the "sandwiched in" QRS complex. She was started on isoprenalin (isoproterenol).
C ASE C onclusion : I lack detailed follow-up from today's case — other than knowing that the Atrial Tachycardia was controlled. This type of Wenckebach response that may be seen with atrial tachycardia ( or atrial flutter ) — is often physiologic, as a result of the rapid atrial rate that occurs with these arrhythmias.
A 50-year-old woman was referred to our hospital for catheter ablation of a regular narrow QRS tachycardia with a short RP interval. No retrograde dual atrioventricular (AV) nodal physiology was observed. A narrow QRS tachycardia was reproducibly induced by programmed atrial extrastimuli with an AH interval jump.
Physiologically — the most commonly observed pattern of AFlutter, known as " Typical " AFlutter — produces 2:1 negative deflections seen in the inferior leads ( as seen in Figure-3 ) — as a result of CCW ( C ounter C lock W ise ) rotation of a fixed reentrant circuit around the tricuspid valve annulus and through the cavo-tricuspid isthmus.
Then, the current flows to an area known as the bundle of His, which divides into two branches (LBB and RBB) and is the only physiological pathway connecting the atria with the ventricles. Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia. Usually does not exceed 160 bpm.
A 68 year-old man underwent diagnostic electrophysiologic study because of a symptomatic short RP supraventricular tachycardia (SVT). Programmed atrial extrastimulation elicited dual atrio-ventricular nodal physiology. Transthoracic echocardiography was normal.
Abstract Introduction Dual atrioventricular nodal non-reentrant tachycardia (DAVNNT) is a rare and challenging-to-diagnose arrhythmia, without previous reports associating it with a leftward inferior extension (LIE). Methods Diagnosis was made using adenosine triphosphate (ATP) injection during atrial pacing in a suspected DAVNNT patient.
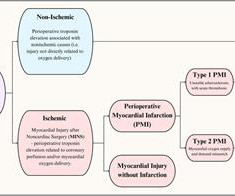
It is frequently driven by physiologic factors such as hypotension, tachycardia, and anemia. Perioperative myocardial injury is a relatively common complication after noncardiac surgery associated with significant morbidity and mortality.
BackgroundPregnancy increases the risk of supraventricular tachycardia (SVT) due to physiological changes. This study reviews the management of SVT in pregnant patients in the emergency department (ED).MethodsWe
A 74-year-old man with a heterotopic heart transplant experienced alternating episodes of sustained native heart ventricular tachycardia and prolonged asystole. The unique physiology in such patients lends itself to numerous clinical considerations that would otherwise be routine management for most.
The Role of Wearable Technology in Heart Health Wearable tech is designed to monitor physiological data and provide actionable insights to users. Early detection of conditions like AFib, bradycardia, or tachycardia allows patients to address issues before they become critical.
Introduction:Supraventricular tachycardia (SVT) is common and poorly tolerated in patients who have undergone Fontan procedure. Atrial Tachycardia (70%) and Typical Atrial Flutter (65%) were the most common SVTs ablated. Circulation, Volume 150, Issue Suppl_1 , Page A4142266-A4142266, November 12, 2024.
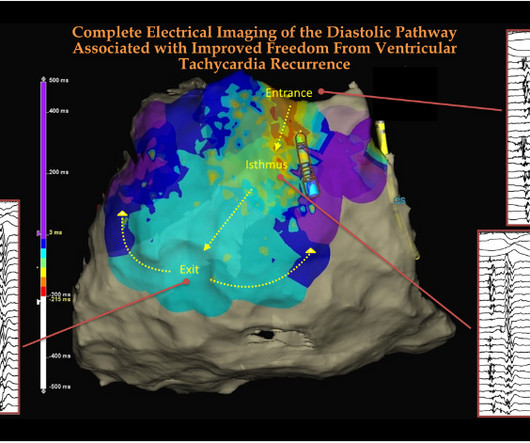
Like hemodynamics of blood , an “electro-dynamic” flow cycle exists that is critically important both in physiology and pathology. Now in modern electro-physiology, it is time to teach young cardiology fellows a new rule of thumb, always look for the (mid )diastolic electrical flow in any scar-induced VT. 2020;13:e008651.
2) Tachycardia to this degree can cause ST segment changes in several ways. First , there can simply be diffuse ST depressions (which obligates reciprocal STE in aVR) associated with tachycardia which are not indicative of ischemia. Sometimes you must correct the rhythm to see what lies underneath. Is this inferor STEMI?
Those with sinus tachycardia were treated with beta-blockers and those with ventricular hypertrophy received a beta-blocker and ACE-inhibitor combination. One manifest physiological, sinus pauses >3.5 s during sleep and another had one asymptomatic episode of non-sustained ventricular tachycardia.
Tachycardia and ST Elevation. Tachycardia to this degree can cause ST segment changes in several ways. First, there can simply be diffuse STD (which obligates reciprocal STE in aVR) associated with tachycardia, which are not even necessarily indicative of ischemia. Christmas Eve Special Gift!! Is this inferor STEMI?
From afar, there is gross tachycardia, cadence irregularities, and narrow QRS complexes that may, or may not, be Sinus in origin; and finally – a cacophony of wide complexes that might very well be ventricular in origin. McLaren : We’ve answered the first question – Sinus Tachycardia with episodic runs of wide QRS (RBBB morphology) and PVC’s.
Physiologic resynchronization by LBBAP may be associated with lower risk of arrhythmias compared with BVP. The incidence of AF lasting >24 hours was also significantly lower with LBBAP compared with BVP (0.7% Conclusions:LBBAP was associated with lower incidence of sustained VT/VF and new-onset AF compared with BVP.
The findings include sinus tachycardia, characteristic QRS morphology most diagnostic in V3 with a small R wave followed by a very large S wave with a convex upward ST segment morphology, ST segment strain morphology in the inferior and anterior leads leading to deep symmetric T-wave inversion. and tachycardia, 1.8. incomplete RBBB 1.7
The ECG accurately reflects the physiologic state of the underlying myocardium, but there is always more than one possible etiology of that physiologic state. Tachycardia is of course, quite common in patients following cardiac arrest. As a result — the history will often be limited to what was known prior to the arrest.
The atrial rate is around 120 beats per minute, which indicates high adrenergic state and physiologic distress! This is sinus tachycardia (rhythm) with complete heart block (AV node function) with ventricular escape rate just below 30. Never forget that sinus tachycardia is the scariest arrhythmia.
Tachycardia (or nearly) 2. Tachycardia, = 1.8. Finally , they found these independent predictors of PE: Note that tachycardia only has an Odds ratio of 1.8. Tachycardia is unusual in ACS unless there is cardiogenic shock or a second simultaneous pathology. Some providers were worried about ACS because of this ECG.
The follow-up ECG ( done ~6 hours after ECG #1 ) — supports my suspicion regarding the physiologic sequence of events in today's evolving OMI ( and provides the likely explanation for why frank ST elevation was not seen in ECG #1 ). There is sinus tachycardia at 100-105/minute. Figure-1: Comparison of the first 3 ECGs in today's case.
2] But there is also Sinus Tachycardia! Physiology. Chapter 4: Cardiovascular Physiology. This is critical for the EMS provider, or ED clinician, as identification of Grade I ischemia (aka, HATW’s) addresses the culprit lesion at the earliest opportunity with excellent downstream prognosis for the patient. [2] 3] Costanzo, L.
(Ken Grauer points out that this 5th beat appears to be due to an early atrial beat and that these early beats continue for a few beats, suggesting a short run of atrial tachycardia.) The 6th beat (the one with the 5th visible pacer spike) has a pacing spike in the midst of the QRS. The pacemaker is not always "right".
The shortened PR-interval, specifically, proved to be quite beguiling as it swept crews down a differential diagnosis of intermittent accessory pathway syndrome – insomuch as a “syndrome” of recurrent tachycardia to account for the patient’s symptoms. Conversely, some patient’s simply have brisk AVN conduction, which is completely benign.
I learned more about the history: 30-something African American with 5-7days of sharp R-sided shoulder/scapula/chest discomfort, presented with sinus tachycardia. Definitive diagnosis is by MRI. This history of a week of constant chest pain is also much more suggestive of myocarditis. OMI it is very unlikely with a week of constant pain.
One looks for sinus tachycardia and diffuse low voltage but many conditions produce these nonspecific findings. Physiologically the ECG finding of electrical alternans correlates with the presence of a swinging heart within the pericardial sac on Echo.
Any alteration in physiology can change "compensated" AS to "decompensated" AS. Inotropes and Vasopressors: Review of Physiology and Clinical Use in Cardiovascular Medicine. Hypotension may of course be a result of a brady- or tachydysrhythmia. 2) Hypoxia, including poisons of oxidative phosphorylation such as HS, CO, CN. Circulation.
Although the shock is no doubt partly a result of poor pump function, with low stroke volume, especially of the RV, it should be compensated for by tachycardia. Cardiac output is stroke volume x rate, so this patient needs a higher heart rate. This is a perfect indication for atropine.
Introduction:Postural orthostatic tachycardia syndrome (POTS) is a chronic syndrome with symptoms of orthostatic intolerance, tachycardia, and exercise intolerance. Circulation, Volume 150, Issue Suppl_1 , Page A4140020-A4140020, November 12, 2024.
Did YOU Notice that the underlying rhythm in Figure-1 appears to be atrial tachycardia? For physiologic reasons, recent years have seen a tendency to favor RV pacing from a higher site in the right ventricle. NOTE #2: I always like to look for the presence of an underlying rhythm in pacemaker tracings.
If the patient has Abnormal Vital Signs (fever, hypotension, tachycardia, or tachypnea, or hypoxemia), then these are the primary issue to address, as there is ongoing pathology which must be identified. Fourth, syncope in the elderly often results from polypharmacy and abnormal physiologic responses to daily events.
Conduction system pacing" is a newer technique that is being studied as a way of delivering more physiologic pacing, typically by inserting a lead into the area of the left bundle branch, or the bundle of His. Additionally, the patient had no other apparent reason to have sinus tachycardia (such as volume depletion, bleeding, fever).
It doesn’t require any extraordinary intelligence to conclude any chronic focal atrial tachycardia can get degenerated to AF in the long run. In that case, the famous atrial tachycardia localizing map from Peter Kistler et al from Australia JACC 2006 holds good for location AF focus too.
It needs a good knowledge of anatomy, physiology of inter & Intra valvular hemodynamics.It It needs a good knowledge of anatomy, physiology of inter & Intra valvular hemodynamics.It Mind you, even an innocuous episode of fever, associated dyspnea, and tachycardia can elevate the mitral gradient and sound a false alarm.
The CASE Continues: The patient had many episodes of NSVT ( Non-Sustained Ventricular Tachycardia ) — like th e one shown below in Figure-6. Learning points : Dual AV physiology in the retrograde direction does not necessarily mean there is dual AV conduction in the antegrade direction. Can YOU identify atrial activity in Figure-6 ?
The physiologic reason for this finding is that the T wave axis in the limb leads generally follows the QRS axis. Removal of any doubt that these inferior lead ST-T wave changes are significant is forthcoming from the abnormal ST segment coving and surprisingly deep T wave inversion in lead aVL ( = reciprocal ST-T wave change ).
Given the immediate physiologic chain reaction of intense autonomic dysfunction that followed on learning of her husband's death ( and which ultimately led to this patients demise ) I have to wonder WHEN ( and How? ) With regard to the Physiologic Chain Reaction As per Dr. Frick We do not have all the answers.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content