This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
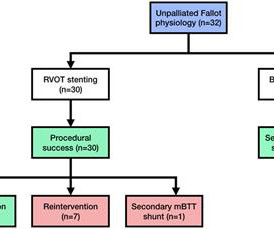
Objectives The purpose of this study was to assess the clinical outcome after right ventricular outflow tract (RVOT) stenting in late presenter patient with unrepaired Fallot physiology. Results During the procedure, the average stent diameter and length were 8.84 ± 1.64 mm The Statistical Package for Social Science (SPSS) 26.0
Welcome to the Physiology Friday newsletter. Physiologically Speaking is a reader-supported publication. Importantly, all of the participants had recently undergone percutaneous coronary intervention (PCI) — a surgical procedure in which a stent is placed in a coronary artery to open up a blockage.
A man in his mid 60s with history of CAD and stents experienced sudden onset epigastric abdominal pain radiating up into his chest at home, waking him from sleep. It is stented with good angiographic result. This patient in today's case was a man in his 60s with a known history of coronary disease, including prior stents.
Together, the two companies will work to further the development and commercialization of Medis Quantitative Flow Ratio (Medis QFR), a non-invasive approach to the assessment of coronary physiology, as part of GE HealthCare’s interventional cardiology portfolio built around the Allia Platform.
The clinical impact of correct assessment of coronary artery stenosis in AF is especially high, due to the antithrombotic therapy imposed by both AF and coronary stenting. Until recently, an in‐depth characterization of coronary microcirculation in AF was lacking.
After significant workup and diagnostic testing, it was believed that he had late complications often seen in Fontan physiology, notably hepatic fibrosis, lymphatic leakage, and protein losing enteropathy. A liver biopsy showed hepatic fibrosis and pleural studies were consistent with chylothorax.
We sought to investigate the association between coronary artery disease patterns, defined by coronary physiology, and optical coherence tomography after stent implantation in stable patients undergoing PCI.Methods and ResultsThis multicenter, prospective, single‐arm study was conducted in 5 countries (NCT03782688). mm2versus 5.19±1.72
But it need not imply the actual functional significance of the stenosis in terms of flow physiology. If the FFR normalizes after stenting, the restenosis rates at six months is less than 5%. Routine FFR measurement probably lead to more judicious use of stents and improved outcomes. Cut off FFR was 0.8 in the study.
On the combined basis of angiography and IVUS, this patient received stents to his mid RCA, proximal PDA, and OM. RCA and PDA before and after, arrows indicating stented regions. OM before and after, arrow indicating stented region. Additional findings: No ST elevation." The basic facts are these: Morphine works.
The Tigertriever stent‐retriever (Rapid Medical, Yokneam, Israel) is a novel operator‐adjustable device that can be actively expanded and contracted by the operator [1], which allows for several actuation‐related parameters to be optimized to potentially improve device efficacy.
It must have re-occluded between the ED and the cath lab) --Lesion was stented. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. Here is the angiogram: --Culprit is 100% stenosis in the proximal RCA. (It Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.)
For a detailed review of deWinter OMI visit this post-- [link] Dr. Stephen Smith provides an academic hypothesis concerning the true underlying physiology of deWinter occlusion here-- [link] The clinical significance of HATW's can be found here-- [link] Crews administered 324 mg of ASA and a total of 0.12 Physiology. 2] Costanzo, L.
After angioplasty (Gateway PTA Balloon Catheter 3.5x20mm, Boston Scientific) and stenting (Wingspan 2.5mmx15mm, Stryker) were performed the residual stenosis was <10% (Figure 1). mL/min.ConclusionThe developed ICAD model is anatomically accurate and offers realistic physiological and procedural features.
Cath done around 4pm next afternoon: Acute culprit lesion: LCX 99%, TIMI 1 flow, stented Also LAD 50%, TIMI 3 flow, which was also stented And chronic RCA occlusion with collaterals (no information is in the cath report regarding where the collateral flow is from, for example if collateral flow was from the LAD or LCX).
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. AV synchrony and physiologic ventricular depolarization the hemodynamics improved. She also has a hx of paroxysmal atrial fibrillation and is on oral anticoagulant treatment. The last echocardiography 12 months ago showed HFmrEF.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. Another factor to be considered, according to Chou’s textbook, is that many patients have dual AVN physiology and conduction is preferential down the fast pathway.
It was stented. == MY Comment by K EN G RAUER, MD ( 9/27/2019 ): == As suggested by the title of this Blog post — confirmation of the diagnosis in this case was made not by ECG — but instead by chest aorta CT ! It just doesn’t make good physiologic sense for there to be an rSr’ only in lead V2, and not in V1.
This case represents the same physiologic event as OMI in terms of the result on the myocardium, therefore with identical ECG features, however there may not be ACS! So you do care what the rhythm is, and you should be wondering: Am I being fooled into seeing ST elevations due to possible flutter waves? ng/mL over the next 10 hours.
It is also unique because it works using the Doppler effect, you can get not only an anatomical evaluation of the heart but also physiological assessment. An echo is easy to do, risk free and easily accessible. It is operator dependant and requires specialised machinery The images you get may vary from patient to patient.
Compare to the anatomy after stenting: The lower of the 2 now easily seen branches is the circumflex, now with excellent flow. In addition — Morphology of the QRS complex and ST-T wave of lead V3 does not make physiologic sense in ECG #1 , considering the relative size and shape of the QRST complex in neighboring leads V2 and V4.
He was successfully stented. He was taken to the cath lab and underwent emergent intervention: Thrombotic stenosis of the proximal RCA (95% with evidence of plaque rupture) is the culprit for the patient's inferoposterior STEMI.
28, 2024 – Elixir Medical today announced late-breaking data demonstrating significant benefit of the DynamX Coronary Bioadaptor System compared to contemporary Resolute Onyx zotarolimus drug-eluting stent (DES) for target lesion failure (TLF) in complex patient population subsets from the INFINITY-SWEDEHEART RCT.
28, 2024 – Elixir Medical today announced late-breaking data demonstrating significant benefit of the DynamX Coronary Bioadaptor System compared to contemporary Resolute Onyx zotarolimus drug-eluting stent (DES) for target lesion failure (TLF) in complex patient population subsets from the INFINITY-SWEDEHEART RCT.
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
The thrombus was aspirated and the distal RCA was stented. The physiologic reason for this finding is that the T wave axis in the limb leads generally follows the QRS axis. The patient waited another three hours in the ED until the cath lab was ready to accept him. There was TIMI 2 flow distal to the thrombotic occlusion.
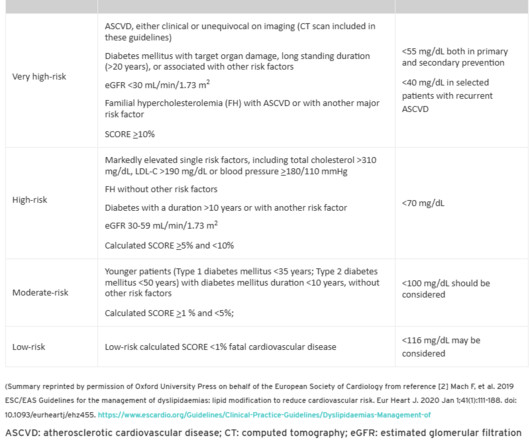
Optimal low-density lipoprotein is 50 to 70 mg/dl: lower is better and physiologically normal. By the way, PREVENT study demands an OCT for all non-flow limiting plaques, and stents if they are found be vulnerable.( Also like subcategorization of clinical ASCVD from image-based ASCVD with reference to target LDL? Reference 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content