This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A significant proportion of patients with severe aortic stenosis (AS) undergoing transcatheter aortic valve implantation (TAVI) have concomitant coronary artery disease (CAD). A better understanding of how we assess and interpret coronary physiology in these patients is required to optimise treatment pathways.
Coronary physiology assessment, including epicardial and microvascular investigations, is a fundamental tool in the contemporary management of patients with coronary artery disease. However, revascularisation of coronary stenosis, which induces myocardial ischaemia, has demonstrated better outcome than OMT alone.
The clinical impact of correct assessment of coronary artery stenosis in AF is especially high, due to the antithrombotic therapy imposed by both AF and coronary stenting. Until recently, an in‐depth characterization of coronary microcirculation in AF was lacking.
Introduction Congenital tracheal stenosis (CTS) is a rare but life-threatening disease that can lead to respiratory dysfunction in children. The order of correction for CTS or OSAS greatly affected the aerodynamic parameters and turbulence flows downstream of tracheal stenosis and upstream of epiglottis.
Coronary computed tomography angiography (CCTA) was a major advancement in CAD diagnostics, helping physicians estimate if a stenosis was significant and requiring intervention. Technologies like Heartflow fractional flow reserve computed tomography (FFR CT ) provide lesion-specific physiology, which enhances CCTAs diagnostic accuracy.
Our objective is to use human-based, tissue-engineered microvessel models to capture these details in response to stenosis, a hallmark of ischemic stroke.Methods:Pluripotent stem cells were differentiated into BMECs (iBMECs), validated for BBB phenotype, and seeded into 150 m channels in collagen I/Matrigel hydrogels.
3% sodium alginate solution was cast into a stenosis mold and crosslinked in a 40% calcium chloride. After angioplasty (Gateway PTA Balloon Catheter 3.5x20mm, Boston Scientific) and stenting (Wingspan 2.5mmx15mm, Stryker) were performed the residual stenosis was <10% (Figure 1).
6 This novel study marks a significant milestone in the field, evaluating the effectiveness of FFR CT in detecting ischemia-producing coronary stenosis in patients with severe PAD. 5 Revascularization to improve blood flow to the heart has been shown to reduce mortality in stable chest pain patients.
Coronary angiography gives a visual impression about the severity of the stenosis. But it need not imply the actual functional significance of the stenosis in terms of flow physiology. A downside of the study was that it had included lesions of 50 to 79% stenosis also. identified physiologically significant stenosis.
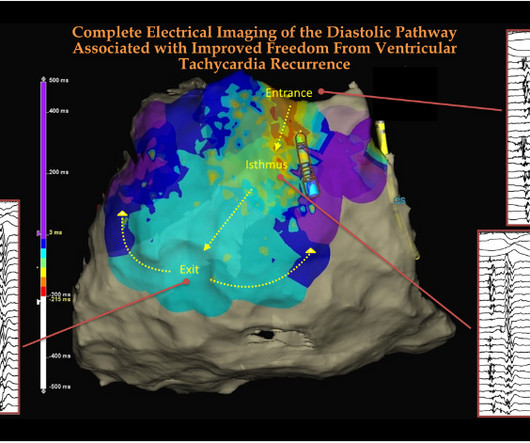
Like hemodynamics of blood , an “electro-dynamic” flow cycle exists that is critically important both in physiology and pathology. Now in modern electro-physiology, it is time to teach young cardiology fellows a new rule of thumb, always look for the (mid )diastolic electrical flow in any scar-induced VT.
Flow is physiology. Sub physiological valve destruction very much possible without affecting gradient. As a cardiologist, very soon we will be allowed legally to choose TAVI even in more younger , low risk cohort of Aortic stenosis without co-morbid conditions. It was not mandatory. Did TEE/CT follow up imaging done ?
Graft material has the disadvantage that it will not grow as the baby grows and can lead to supravalvar pulmonary stenosis later, one of the delayed complications of arterial switch. This is diagrammatic representation of stenosis of pulmonary artery at the site where it has been repaired.
Patient-specific blood flow simulations using physiology-informed boundary conditions calculated stenotic pressure ratios for both the patient’s acute and a population-based healthy scenario. Mean±standard deviation of stenosis degree (SD) 55±14% for patients across each cohort was A) 50±11%, B) 70±9%, C) 70%.
A transthoracic echocardiogram showed an LV EF of less than 15%, critically severe aortic stenosis , severe LVH , and a small LV cavity. The aortic valve in this example also had critical stenosis by Doppler The patient continued to be hemodynamically unstable with poor cardiac output and very high LV filling pressures.
Sensitivity analysis was done by cardiac risk factors, degree of stenosis and image quality. Future research is required to evaluate the physiological relevance and prognostic value of FFR CT. Intraclass correlation coefficient (ICC) and Bland-Altman analysis were used to evaluate interoperator variability effect in FFR CT estimates.
The LAD has diffuse disease with a few areas of moderate stenosis but no flow-limiting lesions. Additional findings: No ST elevation." Again, the spine is off the screen to the left, and the heart is to the right of it. Here we see the LAD , diagonal branches , and the distal LCx. From angiography, it is not clear what the culprit is.
BACKGROUNDHypertension is often codiagnosed in patients with moyamoya disease (MMD), a progressive intracranial steno‐occlusive vasculopathy; this has principally been attributed to renal artery stenosis (up to 10%).
Here is the angiogram: --Culprit is 100% stenosis in the proximal RCA. (It Then the ED doc would be dependent on that first ECG. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. It must have re-occluded between the ED and the cath lab) --Lesion was stented.
We present this case as evidence of a similar angiogenic physiologic response in humans to minimize the microvascular ischemic injury from chronic cocaine use.
The combination of prolonged QT and deep T wave inversion throughout the precordium is typical of Takotsubo syndrome, or Stress Cardiomyopathy – which can occur in the context of a physiologically distressed ICU patient, further compromising their hemodynamics. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration.
That condition is tricuspid stenosis, which is rare. PEARL #3: There is a physiologic reason why pulmonary hypertension from advanced RVH may result in a qR pattern in lead V1 ( Figure-2 ). RAA ( Right Atrial Abnormality ): The tall, peaked and pointed P wave in each of the inferior leads ( ≥2.5
He was taken to the cath lab and underwent emergent intervention: Thrombotic stenosis of the proximal RCA (95% with evidence of plaque rupture) is the culprit for the patient's inferoposterior STEMI. Before transport, a final ECG was recorded: There is, again, inferior reperfusion, but persistent marked anterior STE.
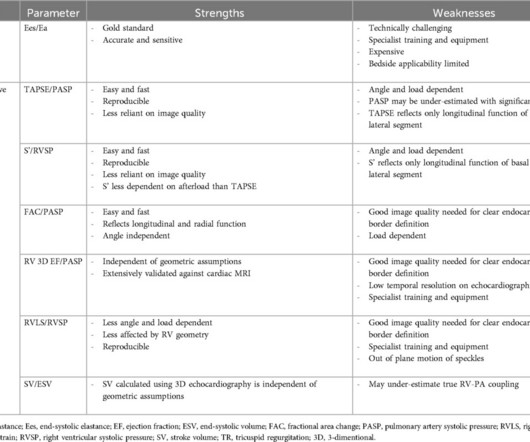
Aortic stenosis (AS) was historically considered a disease of the left side of the heart, with the main pathophysiological impact being predominantly on the left ventricle (LV). This review will summarise the features of normal RV physiology and the mechanisms responsible for RV impairment in AS.
A comprehensive physiological assessment was performed using both a thermodilution-based diagnostic guidewire and intracoronary acetylcholine provocation testing. Angiograms were examined for luminal stenosis in each segment of the SYNTAX coronary model. Angiographic analyses were performed blind to coronary physiology findings.
The FFRangio System obtains physiologic information from routine angiograms, eliminating the need for drug stimulation and invasive pressure wires. The PROVISION Study is the first Japanese prospective RCT comparing the outcomes of an angio-based physiology technology in comparison to invasive wire-based physiology.
Hemodynanmic of normal delivery Natural delivery involves the physiological stress of labor, which includes increased cardiac output, blood pressure fluctuations, and oxygen demand, peaking at 50-80% above baseline during contractions and pushing. In women with significant heart disease, the physiological demands of labor (e.g.,
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content