This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The use of physiology-guided complete revascularization is superior to a culprit-only strategy for older patients with either STEMI or NSTEMI, according to a prespecified substudy of the FIRE trial presented at ESC Congress 2024 in London and simultaneously published in JACC.
Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI. MRR = (CFR/FFR) × (P a,rest /P a,hyper ) References Michel Zeitouni, Ghilas Rahoual, Gilles Montalescot, and the ACTION study group. J Am Coll Cardiol. 2024 May, 83 (21) 2077–2079. van Leeuwen, Stephen P.
Objectives To ascertain whether invasive assessment of coronary physiology soon after recanalisation of the culprit artery by primary percutaneous coronary intervention is associated with the development of microvascular obstruction by cardiac magnetic resonance in patients with ST-segment elevation myocardial infarction (STEMI).
She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI. Respect physiology. Gallbladder ultrasound was negative for stones.
The goal of the FULL REVASC trial was to evaluate physiology-guided complete revascularization compared with usual care among patients with ST-segment elevation myocardial infarction (STEMI) and multivessel coronary disease who underwent culprit-vessel percutaneous coronary intervention (PCI).
There is sinus rhythm with minimal STE in V1-V3, not meeting STEMI criteria. Learning Points: Serial ECGs can sometimes turn a difficult decision into a very easy one, but not all OMIs will develop into clear STEMIs quickly, and some OMIs never will manifest STEMI at all.
Current international clinical practice guidelines recommend complete revascularization for patients with ST-segment elevation myocardial infarction (STEMI) with multivessel coronary artery disease1 on the basis of evidence from randomized, controlled trials.2
Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.) The cath lab was activated prehospital But imagine if the patient had walked in.
SCM may happen from a wide variety of psychological or physiological stresses, including respiratory failure (although in this case a psychological stress led to poor myocardial function and then pulmonary edema, then respiratory failure) and intracranial bleeding. In this case, the ECG never mimicked a STEMI.
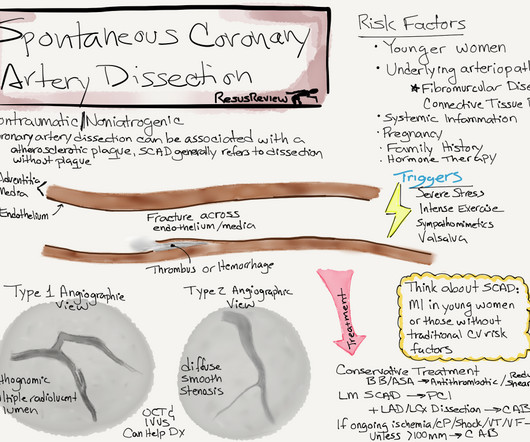
This has important clinical significance , as many successfully lysed STEMI patient might have minimal segments of dissection/deep plaque fissures. , Spontaneous coronary dissection vs Iatrogenic dissection SCAD is a rare , different entity , enjoys a popular space in the patho-physiology of CAD.
Background:5-Hydroxytryptophan (5-HTP) is a natural amino acid and precursor to serotonin, which is essential for various physiological functions. Conclusion:Higher 5-HTP levels are independently associated with a reduced risk of MACE in patients after STEMI. years, 53 women) followed for up to 15 years.
In contrast — it is EASY to overlook L A- L L reversal — because the ECG picture seen with this type of lead reversal does not immediately stand out as physiologically “off”. P utting I t A ll T ogether : After correcting for LA-LL lead reversal — ECG # 1a shows sinus rhythm — LVH — and an acute infero-postero STEMI with acute RV involvement.
Is this inferor STEMI? Atrial Flutter with Inferior STEMI? Inferolateral ST elevation, vomiting, and elevated troponin The treating team did not identify the flutter waves and they became worried about possible "STEMI" (despite the unusual clinical scenario). The EM provider asked if the cardiologist thought it was a "STEMI."
The computer read Anterior STEMI along with RBBB. I would activate the cath lab based on this and the clinical presentation, but I do NOT see any evidence of anterior STEMI The patient arrived in the ED and had this ECG: The T-waves are now less hyperacute, but ST Elevation remains. Here is his prehospital ECG: What do you think?
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. Serial echo monitoring showed increasing pericardial pressures without overt tamponade physiology. Of note, there is arguably terminal QRS distortion in V4-V6. Pericarditis maybe."
Frailty is a syndrome of physiological decline, characterized by marked vulnerability to adverse health outcomes. Over 600,000 percutaneous coronary interventions (PCI) are performed each year for IHD. Frailty and CVD are often interrelated, affecting disease and treatment outcomes. Frailty is prevalent in adults with IHD requiring PCI.
And, the drug does provide physiologic benefits for a patient with an acute cardiac event ( ie, it helps to relieve anxiety as well as pain — which may decrease activation of autonomic nervous system activity — often resulting in reduced heart rate, blood pressure, venous return and myocardial oxygen demand — Murphy et al: StatPearls, 2023 ).
Another factor to be considered, according to Chou’s textbook, is that many patients have dual AVN physiology and conduction is preferential down the fast pathway. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. The shortened PR-interval is probably an accessory pathway.”
There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI). Physiology. Chapter 4: Cardiovascular Physiology. 2] Costanzo, L. Elsevier: Philadelphia, PA. [3]
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. EKG is pictured below: What do you think?
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. Then, three minutes later… Crews activated STEMI as she deteriorated into PEA arrest. Physiology. Chapter 4: Cardiovascular Physiology. 3] Costanzo, L. 4] Parham, W.
Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. Is this a transient STEMI? Is it normal ST elevation?
The axiom of "type 1 (ACS, plaque rupture) STEMIs are not tachycardic unless they are in cardiogenic shock" is not applicable outside of sinus rhythm. This case represents the same physiologic event as OMI in terms of the result on the myocardium, therefore with identical ECG features, however there may not be ACS!
Diagnosis: Acute non-ST segment elevation MI (Non-STEMI, or NSTEMI) Second troponin returned at around 0200: 15,894 ng/L 0245 (unclear if ongoing pain or not) Inferoposterior (and lateral V5-6) reperfusion findings. Admitted to the hospital service for further evaluation and management."
But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. Still no WPW pattern, and more obvious inferoposterior OMI, but still STEMI negative. The emergency physician wasn’t sure what to make of the changes from one ECG to the next but was concerned about ACS. What do you think?
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 The atrial rate is around 120 beats per minute, which indicates high adrenergic state and physiologic distress! What do you think? mm STE in V2). The Queen of Hearts also sees no OMI with high confidence.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. Any alteration in physiology can change "compensated" AS to "decompensated" AS. What do you see?
Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI. For some reason (with debatable physiology), coronary occlusion often causes decrease in the high voltage of LVH on the EKG. I took part in her ICU care and she was extubated and stable to transfer to a stepdown unit after a few days.
But lead V2 has a worrisome amount of ST elevation, and in a chest pain patient, I would be worried about STEMI. My subjective interpretation, and that of Pierre's, is of LVH with secondary repolarization abnormalities, including pseudoSTEMI ST elevation in V1-V3. The Ratios of STE to S-wave: V1: 2.5/16
The ECG accurately reflects the physiologic state of the underlying myocardium, but there is always more than one possible etiology of that physiologic state. He had multiple cardiac arrests with ROSC regained each time.
This paper by Bischof and Smith compared inferior MI to pericarditis and found that of 154 patients with inferior STEMI, 17% of whom had less than 1 mm of STE in any inferior lead, all 154 had at least 0.25 Maybe an increase in pericardial fluid could have been observed and helped to prevent her acute decompensation one week later.
In addition — Morphology of the QRS complex and ST-T wave of lead V3 does not make physiologic sense in ECG #1 , considering the relative size and shape of the QRST complex in neighboring leads V2 and V4.
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." As the troponin T was 1521 ng/L (peak troponin T over 1000 ng/L is typical of STEMI) and still rising, no further troponins were measured. How does the Queen of Hearts do?
When interpreting ECGs such as the initial tracing in today's case We need to remember that we are not trying to "rule in" an acute STEMI. Physiologically this may occur as a result of very brief coronary occlusion, followed so soon after by spontaneous reperfusion. What do these Subtle Findings Mean?
His first EKG is shown below, with a lead II rhythm strip: EKG 1, 1645 A provisder who is looking for STEMI would not see much in this EKG. It is possible that the T waves in this EKG are of an intermediate morphology between full-blown STEMI and inferior reperfusion. This is the classic morphology of hyperacute T waves.
Given the immediate physiologic chain reaction of intense autonomic dysfunction that followed on learning of her husband's death ( and which ultimately led to this patients demise ) I have to wonder WHEN ( and How? ) With regard to the Physiologic Chain Reaction As per Dr. Frick We do not have all the answers.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content