This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This ECG is diagnostic of anterior STEMI. But there was some doubt as to whether it might be pericarditis because of the ST elevation in I and II, without ST depression in III. Add that to "sharp" pain and a 33 year old, and it is easy to convince yourself that this is, indeed, pericarditis. However, look closely!
The patient was discharged with a diagnosis of acute pericarditis — and treated with a full course of colchicine and ibuprofen. The ultimate discharge diagnosis was acute pericarditis. ( From the information provided — I would not make the diagnosis of acute pericarditis. Figure-1: The initial ECG in today's case.
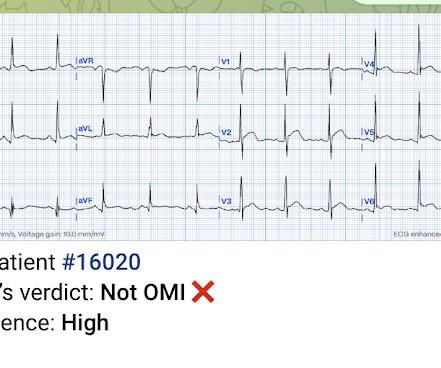
Below is the first ECG, signed off by the over-reading cardiologist agreeing with the computer interpretation: ST elevation, consider early repolarization, pericarditis, or injury. Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury.
Overall, this looks like one of the rare ECGs that is actually specific for pericarditis in my opinion. QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. Pericarditis maybe." There was no prior ECG for comparison.
This ECG together with these symptoms is certainly concerning for OMI, but the ECG is not fully diagnostic, and another consideration could be acute pericarditis. Mistaking OMI for pericarditis is a much more harmful error than the converse. The rate is tachycardic, which is uncommon in OMI and common in pericarditis.
The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.” The final cardiology interpretation confirmed the computer interpretation of “ST elevation, consider early repolarization, pericarditis or injury”. A healthy 45-year-old female presented with chest pain, with normal vitals.
mm has been described in normal subjects) Overall impression: In my opinion and experience, this ECG most likely represents a normal baseline ECG, but with a small chance of pericarditis instead. I texted this to Dr. Smith without any information, and this was his reply: "This could be pericarditis but probably is normal variant."
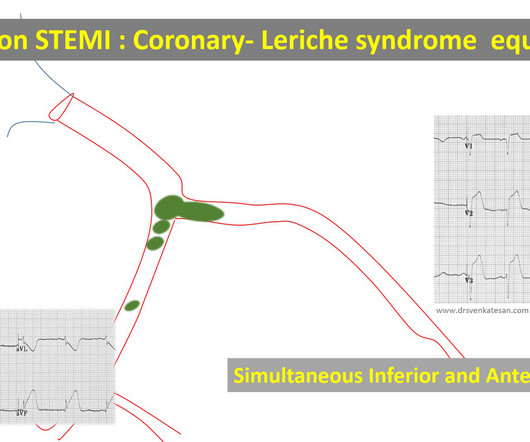
True bifurcation STEMI with static thrombus (Carinal trapping of thrombus ,Coronary Lerish sydrome ) 4. Embolic STEMI with showers of emboli into both LCX and LAD Simultaneous or sequential Anterior and Inferior STEMI 5. Wrap around LAD true Global MI 2. RCA-dependent LAD circulation through collaterals 3.
Jesse McLaren guides us through 9 cases and explains how pericarditis is a diagnosis of exclusion through 3 simple steps: 1. Exclude complications of pericarditis, eg myocarditis, large pericardial effusion 3. The post ECG Cases 27 Pericarditis – Diagnosis of Exclusion appeared first on Emergency Medicine Cases.
Clinician and EKG machine read of acute pericarditis. While it is true that inferior MI has ST depression in aVL 99% of the time (Bischof and Smith), and that inferolateral ST elevation is the most common distribution for pericarditis, the ST elevation in V3 has "terminal QRS distortion (TQRSD)," (diagnostic of LAD occlusion).
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
Here is his initial ED ECG: The R-wave in V4 extends to 33 mm, the computerized QTc is 372 ms The only available previous ECG is from one year ago, during the admission when he was diagnosed with pericarditis: 1 year ago ECG, with clinician and computer interpretatioin of pericarditis Normal 0 false false false EN-US X-NONE X-NONE What do you think?
06:44 - T-waves in V2 are smaller now - Overall resolution of prior findings (which qualifies as a dynamic change) The initial note by the cardiologist states that the presentation is more consistent with pericarditis. Remember, pericarditis is the thing you say and write down when youre actively trying to miss an OMI.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardial infarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). As already mentioned, this patient could have post-infarction regional pericarditis from a large completed MI. Sinus tachycardia has many potential causes. Hammill SC.
Triage ECG: It was interpreted as lateral STEMI, and he was sent to the cath lab, where the angiogram showed unchanged CAD from known prior, with no acute culprit. Patient 2 A man in his 50s with history of CAD and prior PCI, diabetes, presented with acute constant chest pain for the past few hours. Described as a dull ache, 6/10 in severity.
Jesse McLaren guides us through 10 cases, driving home the points that sepsis is a common cause of rapid Afib and diffuse ST depression with reciprocal ST elevation in aVR, myo/pericarditis is a diagnosis of exclusion, endocarditis or lyme carditis can cause AV block, PE can cause low grade fever and ECG signs of acute RV strain and that fever can (..)
In this ECG Cases blog we look at 10 cases of patients with chest pain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The undergraduate continues: This new EKG pattern is more suggestive of acute pericarditis. Usually with pericarditis, some degree of PR segment depression is expected. This is typical of pericarditis. This EKG seems to lack it.
There is a reasonable chance of pericarditis in this case, or this could be a baseline." Here is the Queen of Heart's interpretation: The cath lab had been activated for concern of STEMI. Sadly, I did not receive enough information to adjudicate whether this patient has pericarditis or not. I immediately responded: "cool fake!
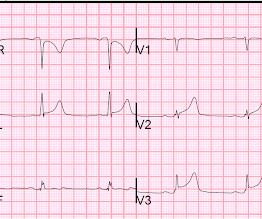
Let's look at the ED ECG more closely: Sinus rhythm There is ST Elevation in anterior leads: V2-V6 There is ST elevation in I, II, aVL Why is this not STEMI? I am reluctant to reverse a diagnosis of STEMI because I would rather there be a false positive cath lab activation than a false negative. No active chest pain 2.
Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." He diagnosed anterior "STEMI" and activated the cath lab. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
PR depression, which suggests pericarditis 4. We also showed that, of 47 cases of pericarditis with ST elevation, none had ST depression in aVL. ) Exclusion criteria were age less than 18, SBP less than 100 mmHg, echocardiogram with EF less than 50%, STEMI, pregnancy, and trauma. Absence of any ST depression in aVL. (
The computer read Anterior STEMI along with RBBB. I would activate the cath lab based on this and the clinical presentation, but I do NOT see any evidence of anterior STEMI The patient arrived in the ED and had this ECG: The T-waves are now less hyperacute, but ST Elevation remains. Here is his prehospital ECG: What do you think?
This ECG clearly meets STEMI criteria by the way, regardless of age or gender. Haven't you been taught that this favors pericarditis? Weren't you taught that concave morphology favors pericarditis? This is a high troponin (most STEMI are above 10 ng/mL for troponin I). There is no STE or STD in III an aVF.
These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. Usually with pericarditis and myocarditis — hyperacute T waves (HATW) are not present.
She was diagnosed with pericarditis and spent one day in the hospital without events. Much more classic findings of pericarditis. Learning Points: Pericardial effusion is a key piece of information for the diagnosis and prognosis of pericarditis. Another ECG was performed, and this time was noted to be markedly abnormal.
The STD in V2-V4 is almost certainly reciprocal STD, reciprocal to STEMI in the posterior wall; this is evident because it is maximal in V2-V4, not in V4-V6. In patients with suspicion of acute MI who have any ST elevation, aVL is also a very useful lead to differentiate between pericarditis and MI. mm ST depression in aVL.
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Is it normal STE? The computer thinks so, and the physician thinks that is quite possible. However , there is terminal QRS distortion in lead V3.
First, many on Twitter said "Pericarditis". This is NOT pericarditis, which virtually NEVER has ST depression any where except aVR. See our publication: ST depression in lead aVL differentiates inferior ST-elevation myocardial infarction from pericarditis There is STE in inferior leads, high lateral leads, and V4-V6.
It could also be due to pericarditis or myocarditis, but I always say that "you diagnose pericarditis at your peril." The clinical presentation is very suggestive of myo-pericarditis. But one should always remember that acute MI is a far more common pathology than myo- or pericarditis. Pericarditis? 13, 2019 Dr.
So Shark Fin really is just a dramatic representation of STEMI, and can be in any coronary distribution. So this is STEMI, right? Well, don't we see diffuse ST Elevation in Myo-pericarditis (with STD in aVR)? It is often confused with a wide QRS due to conditions such as hyperkalemia. Which artery? Could this be myopericarditis?
This morphology can be cause by or associated with cocaine: A Patient with Cocaine Chest Pain and Prehospital Computer interpretation of STEMI This is OMI of the anterior, lateral, and inferior walls until proven otherwise. But it does not meet STEMI criteria and it was not initially recognized. The cath lab was now activated.
It is uncommon in the age of reperfusion therapy, as most STEMI get treated reasonably early, before transmural infarct. Patients with completed, transmural infarct are also at risk for post-infarction regional pericarditis and myocardial rupture. Most STEMI peak at over 10 ng/mL; most NonSTEMI at less than 10 ng/mL.
This is a bad ST vector orientation, because it causes widespread STE and one of the most important mistakes that needs to be avoided here is thinking of the diagnosis of pericarditis. Such an out-of-proportion STE is virtually never seen in pericarditis. Look at the STE in lead II, aVF.
Discharge Diagnosis was STEMI (The STE did not meet "criteria," so "OMI" would be better, but "STEMI" is far better than what this could have been called: NonSTEMI) Quotes from a note written by a really fine and knowledgable physician: "12-lead EKG was obtained initial 1 at time zero. Initial troponin came back negative."
ECG read as: "Shows T wave inversions in the inferior leads and less than 1mm STE in V2, without STEMI criteria." All very very subtle. So the patient was placed back in the waiting room like many others. Aspirin was given. History and more info?" (I What is the South African Flag Sign?
You do NOT see this in normal variant STE, nor in pericarditis. Here is the computer interpretation: (Veritas algorithm) This is what I said: "This is diagnostic of an acute inferior MI. There is upsloping ST elevation in III, with reciprocal ST depression in aVL.
In this ECG Cases blog we look at 8 patients with potentially ischemic symptoms, to highlight pearls and pitfalls of inferior MI. Can you identify which ones had acute coronary occlusion? The post ECG Cases 3: Can you find the subtle inferior MI? appeared first on Emergency Medicine Cases.
In this ECG Cases blog we look at 10 patients who presented with ST elevation, and review the differential diagnosis of ST elevation using the ELEVATIONS mnemonic. Which had occlusion MI? The post ECG Cases 17 – ST ELEVATIONS mnemonic and Occlusion MI appeared first on Emergency Medicine Cases.
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Armstrong et al.)], the presence of such well developed anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content