This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundCryoablation for pediatric atrioventricular nodal reentry tachycardia (AVNRT) is favored for reducing conduction system injury compared to radiofrequency (RF) ablation. Currently, 3D EAM systems offer precise and efficient guidance, improving safety and outcomes.
Abstract Introduction Supraventricular tachycardia (SVT) is a common pediatric arrhythmia. We describe the prescriptive tendencies, efficacy, and tolerability of BBs and CCBs used in the treatment of pediatric SVT. Exclusion criteria were pre-excitation, ectopic atrial tachycardia, and hemodynamically significant heart disease.
Discussion on pediatric exercise testing. Pediatric exercise testing may be used for evaluation of various disorders of cardiac rhythm rather than for inducible ischemia as in adults. Bidirectional ventricular tachycardia is the classical arrhythmia noted in catecholaminergic polymorphic ventricular tachycardia.
Disparities have been shown in the treatment of pediatric supraventricular tachycardia (SVT). The Childhood Opportunity Index (COI) is a validated approach that uses a composite index of 29 indicators of social determinants of health linked to the US Census. The relationship between COI and SVT has not been previously published.
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. During the next 24 hours, she experienced periods of complete AV block with a ventricular escape rhythm in the 20s. She was started on isoprenalin (isoproterenol). The following ECG was recorded during one of these episodes of VT.
ABSTRACT Introduction The aim of this study was to describe our experience and outcome of ablation therapy for arrhythmias in pediatrics at a tertiary care center. All pediatrics presenting to AUBMC between 2000 and 2020 who underwent cardiac ablation were included. The completed procedures showed a success rate of 93%.
It has been used to treat both inappropriate sinus tachycardia and sinus tachycardia related to heart failure in children and adults. Ivabradine’s high selectivity and minimal side effects make it an attractive candidate for wider applications such as focal atrial tachycardia (FAT).
Background:In diabetic ketoacidosis (DKA), cardiac complications such as QTc interval prolongation can pose a risk for ventricular tachycardia. Current pediatric DKA management guidelines should include routine 12-lead ECGs and venous blood gas analyses with electrolytes to monitor QTc changes and mitigate arrhythmia risks.
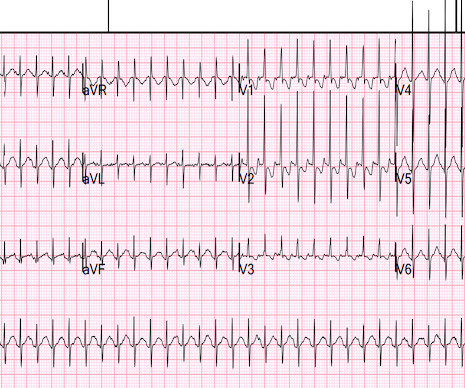
IntroductionFocal atrial tachycardia (FAT) is predominant in the pediatric population. A 12-lead electrocardiogram revealed a narrow QRS complex tachycardia with a rate of 157 beats per minute and a prolonged RP relationship. Echocardiography indicated a severely reduced ejection fraction of 22%.
Objective Describe the methodology and role of CNA for treatment of pediatric patients with functional AVB or SP. with one documented SP after termination of atrial tachycardia at the 3-month follow-up. Methods This is a single-center, case series study. Post-CNA, the median longest pause was 1.3 s s (range 0.8–2.2)
Based on this robust study, one can conclude that symptomatic pediatric CPVT patients are at high risk for arrhythmic syncope, SCA and SCD even when receiving medical treatment. Compliance and underdosing with medications play a major role in these risks. LCSD may be underutilized in CPVT.
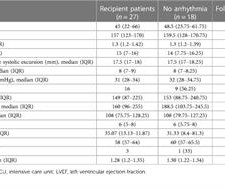
Methods We performed a retrospective clinical data review of all consecutive pediatric patients (aged 2–18 years) who underwent orthotopic HT for advanced heart failure at our institution between January 2007 and January 2023. Clinical, procedural, and follow-up data were collected and comprehensively analyzed.
so it must be a pediatric ECG. The ECG was done because the heart rate was 230 and the differential included SVT vs. sinus tachycardia. This is typical of pediatric ECGs because the fetal circulation depends on the right ventricle. What can you say about this ECG at a rate of 230 beats per minute?
Left cardiac sympathetic denervation (LSCD) is an effective treatment for channelopathies, especially in those where adrenaline acts as a trigger for life-threatening arrhythmias, such as long QT syndrome (LQTS) and catecholaminergic polymorphic ventricular tachycardia (CPVT).
Acute fulminant myocarditis (AFM) presenting with ventricular tachycardia (VT) has been associated with poor early outcome, and complete heart block (CHB) is rare, especially without ventricular escape rhythm.
Here is his 12-lead: There is a wide complex tachycardia with a rate of 257, with RBBB and LPFB (right axis deviation) morphology. Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. See Learning point 1 below.
This is one important cause of supraventricular tachycardia in Ebstein’s anomaly. Ebstein’s anomaly may present with a murmur for evaluation in the pediatric age group or in adults with arrhythmias or heart failure with cyanosis and exercise intolerance.
IF this was 2:1 AV block — then the P-P interval should be everywhere the same ( with only occasional exception of some atrial tachycardias in adults that may not always be completely regular ). It is important to remember that pediatric tracings manifest a number of differences from adult ECGs.
Interpretation: There is sinus tachycardia, with right bundle branch block (RBBB). She was pulseless, with a narrow complex tachycardia on the monitor. She was intubated. A FAST exam was normal (no pericardial or peritoneal fluid). As part of her workup, this ECG was recorded: What do you think?
Otherwise vitals after intubation were only notable for tachycardia. An initial EKG was obtained: Computer read: sinus tachycardia, early acute anterior infarct. Pediatric and elderly patients were more predisposed to developing an arrhythmic event in the setting of fever [7]. A rectal temperature was obtained which read 107.9
It is seldom done in pediatric age group. There is a potential risk for drug challenge in that life threatening ventricular arrhythmias could be precipitated. Hence drug challenge is to be done only in a monitored intensive care facility. With proper precautions, risk can be reduced.
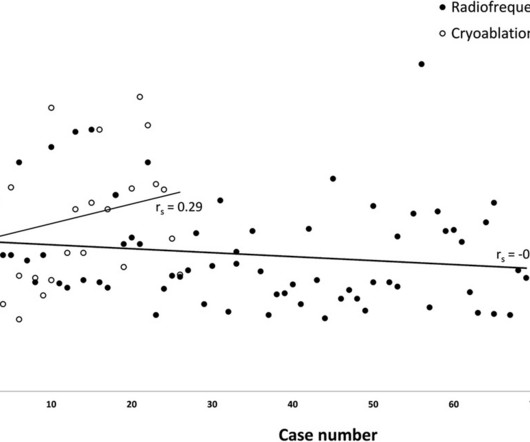
ABSTRACT Background Low voltage bridge mapping (LVBM) is an approach to atrio-ventricular nodal reentry tachycardia (AVNRT) ablation that has been postulated to facilitate the procedure. The aim of this study was to analyze how the introduction of the LVBM influenced the results of the pediatric AVNRT ablations using the RF current.
There is sinus tachycardia and also a large R-wave in aVR. Drug toxicity , especially diphenhydramine , which has sodium channel blocking effects, and also anticholinergic effects which may result in sinus tachycardia, hyperthermia, delirium, and dry skin. Her temperature was 106 degrees. As part of the workup, she underwent an ECG.
PurposeAtrial tachycardia is an uncommon supraventricular tachycardia in children. It is often drug-resistant and likely to occur concomitantly with tachycardia-induced cardiomyopathy, making radiofrequency catheter ablation the preferred treatment. A total of 78.6% No postoperative complications occurred in any patient.
Atrioventricular nodal reentrant tachycardia (AVNRT) is a common supraventricular tachycardia in children and congenital heart disease (CHD) patients. Nowadays, in large enough children, chronic treatment for symptomatic and recurrent AVNRT episodes relies on transcatheter ablation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content