This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Tricuspid valve disease is an often underrecognized clinical problem that is associated with significant morbidity and mortality. This review highlights the important background, anatomic considerations, therapeutic options, and future directions with regard to treatment of tricuspid valve disease. Circulation, Ahead of Print.
Tricuspid regurgitation (TR) is a common and serious disease for which open heart surgery and symptomatic pharmacologic treatment are the current standard treatment options. Importantly, the performance of the pacemaker was not affected by the valve.
Traditional transvenous pacemakers consist of a pacemaker generator usually positioned surgically in the upper left chest on the pectoral muscle fascia and one or more leads positioned through the veins to the right atrium and across the tricuspid valve to the right ventricular apex.
At 30-day follow-up, all-cause mortality, the incidence of major adverse cardiovascular events, major vascular complications, and new permanent pacemaker implantation were 3.8%, 4.6%, 0.8%, and 0.8%, respectively. of patients showedmild paravalvular leakage, and all 125 (100%) patients were in New York Heart Association ClassII.
Tricuspid regurgitation (TR) is a well-known complication after transvenous pacemaker implantation that is less well described for leadless pacemakers (LPs).1 1 Previous studies have reported discordant data regarding the incidence of significant TR with LP compared to transvenous systems.24
Tricuspid valve surgery for isolated tricuspid valve disease is becoming increasingly common. These patients often need permanent pacemaker (PPM) post-surgery. Incidence and risk factors of this complication are not well established.
Tricuspid regurgitation (TR) is a common valvular disorder with a spectrum of etiologies including mechanical disturbance of the tricuspid valve by catheters, wires, and the presence of a pacemaker or defibrillator.
Lead dislodgements, tricuspid valve failure, and wound infections are prominent issues addressed by leadless pacemakers (LPM). These devises have emerged as viable alternatives to conventional transvenous pace.
ABSTRACT Leadless pacemakers as the Medtronic Micra AV, have improved cardiac pacing by reducing complications associated with traditional systems. Right atrial function, particularly the tricuspidal E wave deceleration time, emerged as the only independent predictor of AVS ( p =0.03), with an AUC of 0.77.
Severe Tricuspid Regurgitation (TR) is associated with increased mortality. Change in TR severity with transvenous pacemaker (PPM) and implantable cardioverter defibrillator lead extraction has been poorly studied.
ABSTRACT Introduction Atrial fibrillation (AF) is the most common arrhythmia, and atrioventricular (AV) node ablation with pacemaker implantation is a therapeutic option for refractory cases. However, AV node ablation in patients with bioprosthetic tricuspid valves poses technical challenges.
ABSTRACT Introduction A leadless pacemaker (LLPM) was recommended for a patient with intermittent complete heart block and near-syncope. The LLPM could not traverse the tricuspid valve. Methods and Results Delivery of LLPM is through a large sheath that has limited deflection and steerability.
Written by Willy Frick A man in his 70s with a history of HFrEF and sick sinus syndrome s/p dual chamber pacemaker placement was admitted for overnight observation following outpatient placement of a mitral valve clip. This is unambiguous evidence of pacemaker malfunction. Imagine the pacemaker is set at a minimum rate of 60.
Methods and Results A 78-year-old female with severe tricuspid regurgitation received two TriClip devices. Postprocedure, frequent significant sinus pauses required a pacemaker. HBP was chosen to avoid lead complications. Under local anesthesia, a His pacing lead was inserted via the axillary vein using specialized catheter.
Leadless pacemakers (LP) are being increasingly utilized to avoid complications associated with transvenous pacemakers, such as infection, venous occlusion, tricuspid regurgitation, and lead related complications (dislodgment, fracture, or insulation failure).
The study aims to compare the outcomes of transcatheter aortic valve replacement for AS in patients with type 0 bicuspid, type 1 bicuspid, and tricuspid aortic valve anatomy.METHODS:We enrolled consecutive patients undergoing transcatheter aortic valve replacement for severe AS between 2012 and 2022 in this single-center retrospective cohort study.
Currently, there are no sutureless options available for vessel closure following large-bore venous procedures. Current venous closure methods are not indicated for large hole venous access applications like Transcatheter Edge-to-Edge repair (TEER), TMVR and TTVR.
The increasing adoption of transcatheter tricuspid valve replacement (TTVR) has underscored the complexities of managing patients with cardiac implantable electronic device (CIED) leads and tricuspid valve (TV) interventions.
BACKGROUND:This study aimed to compare the incidence and prognostic implications of new-onset conduction disturbances after surgical aortic valve replacement (SAVR) in patients with bicuspid aortic valve (BAV) aortic stenosis (AS) versus patients with tricuspid aortic valve (TAV) AS (ie, BAV-AS and TAV-AS, respectively).
Tricuspid valve replacement was performed in 26 (53%) patients including 19 (73%) cases of combined pulmonary valve replacement. Epicardial pacemakers were systematically implanted in operated patients and 25% were permanently paced. A postoperative positive right ventricular remodelling was observed (p<0.001).
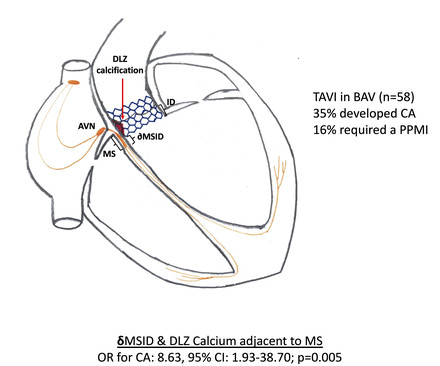
Background TAVI is associated with CA that commonly necessitate a permanent pacemaker. Predictors of CA are well established among patients with tricuspid aortic valves but not in those with BAV. Methods This is a single-centre, retrospective, observational study of patients with BAV treated with TAVI.
Single-arm studies, conference presentations, animal studies, and studies that involved patients with tricuspid aortic morphology were excluded. to 0.63, p=0.01) but a higher risk of new permanent pacemaker placement (RR 2.17, 95%CI 1.03 Medical databases were queried to pool comparative studies of interest. to 4.58, p=0.04).
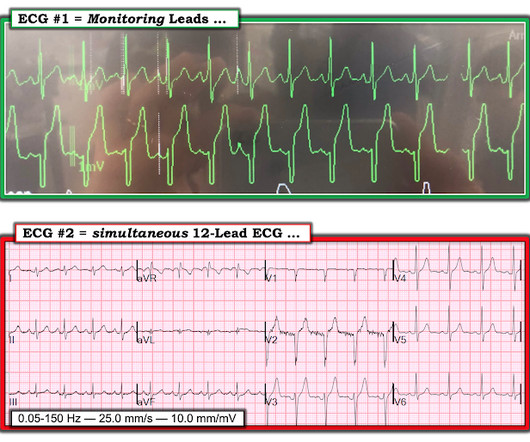
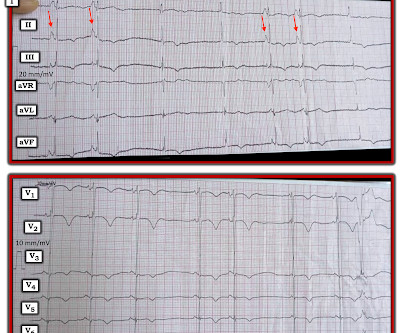
I’d guess the overall rhythm is sinus, perhaps with a wandering atrial pacemaker and very frequent ventricular ectopy with multiple couplets. Perhaps the patient has pulmonary hypertension and/or tricuspid regurgitation? In the meantime, a pacemaker may be needed. =
And that will be the approximate level of the tricuspid valve, the reference point for measuring right atrial pressure. In right atrial tracing, this occurs at the time of right ventricular contraction, with bulging upwards of the tricuspid valve. The Y descent is shallow in tricuspid stenosis, and absent in cardiac tamponade.
Again, see Ken's discussion below) Discussion continued The absence of pace spikes suggests this is not a pacemaker/ICD-related rhythm in this patient with an ICD. This physical exam sign is seen with AV dissociation — and results from right atrial contraction against a closed tricuspid valve. Where does the QRS begin?
BackgroundData regarding permanent pacemaker (PPM) implantation following tricuspid valve surgery (TVS) are limited. Tricuspid valve (TV) replacement was associated with a significantly higher risk of PPM implantation when compared with TV repair (RR, 3.20 [95% CI, 2.16–4.75],P<0.0001). 1.49],P=0.04). 1.12],P=0.7).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content