This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Then I always look to see if the initial deflection of the QRS has a lot of voltage change per change in time (seen in tachycardias that are initiated from above the ventricle because the propagate through fast conducting purkinje fiber. Tachycardia exaggerates ST Elevation in LBBB and Paced rhythm 5. Pacemaker mediated tachycardia!
Typically, patients with HCM experience sinus tachycardia and sinus arrest relatively infrequently. To manage the complex comorbidities, we opted for dual-chamber pacemaker implantation. Meanwhile, a dual-chamber pacemaker can treat HCM by changing the sequence of myocardial contraction.
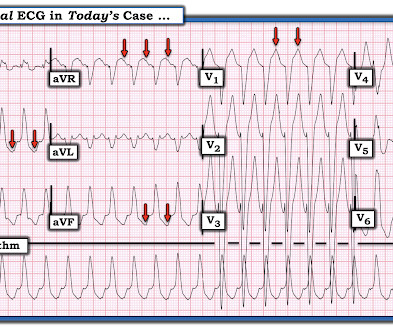
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Answer : The ECG above shows a regular wide complex tachycardia. Said differently, the ECG shows a rather slow ventricular tachycardia with a 2:1 VA conduction. Cardiac output (CO) was being maintained by the tachycardia.
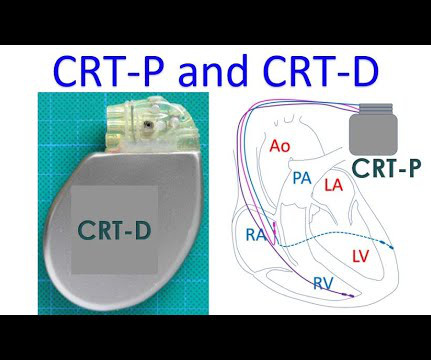
A patient in the ICU with significant underlying cardiac disease [HFrEF 30%, non-ischemic cardiomyopathy, LBBB s/p CRT-D (biventricular pacer), AVNRT s/p ablation a few yrs ago, hx sinus tachycardia while on max tolerated BB therapy] went into a regular wide-complex tachycardia after intubation for severe COPD exacerbation. What to do?
(MedPage Today) -- BOSTON -- A leadless pacemaker reliably communicated with a subcutaneous implantable cardioverter-defibrillator (S-ICD) to deliver anti-tachycardia (ATP) and bradycardia pacing, the MODULAR ATP study showed. In terms of safety.
If ventricular tachycardia occurs in an Implantable Cardioverter Defibrillator (ICD) wearer, the ICD can combat this with 2 different forms of therapy, provided these are activated (which can be done using a programming device). First, the ICD attempts to override the tachycardia. The fastest pacemaker gets control of the heart.
In this month's ECG Cases blog Dr. McLaren explains the PACER mnemonic approach to patients with pacemakers: Pacemaker spike: is it appropriately presence/absent, is there pacemaker-mediated tachycardia (apply magnet) or is there failure to pace (apply magnet to stop sensing, cardio consult)?
If ventricular tachycardia occurs in an Implantable Cardioverter Defibrillator (ICD) wearer, the ICD can combat this with 2 different forms of therapy, provided these are activated (which can be done using a programming device). First, the ICD attempts to override the tachycardia. The fastest pacemaker gets control of the heart.
BackgroundHuman pluripotent stem cell-derived cardiomyocytes (hPSC-CMs) show tremendous promise for cardiac regeneration following myocardial infarction (MI), but their transplantation gives rise to transient ventricular tachycardia (VT) in large-animal MI models, representing a major hurdle to translation.
Place temporary pacemaker 3. Even with tachycardia and a paced QRS duration of ~0.16 Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. See this post: How a pause can cause cardiac arrest 2. Discontinue amiodarone, since it prolongs the QT 4. J Am Coll Cardiol.
The ECG shows an example of a patient with bradycardia/tachycardia syndrome. After a further pause of just under 2000 ms, 2 sinus node beats follow, which merge into a sinus tachycardia or atrial tachycardia (heart rate approx. Initially, a sinus rhythm with a heart rate of approx. 70 bpm is seen. 120 bpm here). 120 bpm here).
Shortly after isoprenalin infusion was initiated, there were short runs of ventricular tachycardia. Isoprenalin was discontinued, and a temporary transveous pacemaker was implanted. The patient stabilized following pacemaker placement. The following ECG was recorded during one of these episodes of VT.
PVC response Atrial-Pace (PVC-A-Pace) is a programmable algorithm developed by Abbott to prevent pacemaker mediated tachycardia after premature ventricular contractions (PVC) in all dual chamber cardiac implantable electronic devices (CIED) (1).
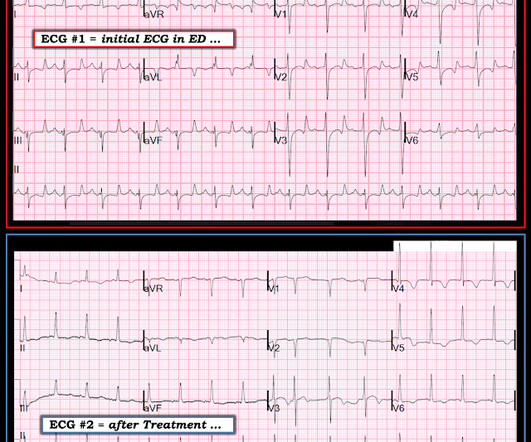
C linical I MPRESSION: I would interpret ECG #1 as suggestive of near ventricular standstill — with underlying atrial tachycardia, extended pauses, and no reliable ventricular escape focus. A permanent pacemaker is needed. = This is often a pre-lethal rhythm. PEARL # 1: The rhythm in ECG #1 is more than just "complete AV block".
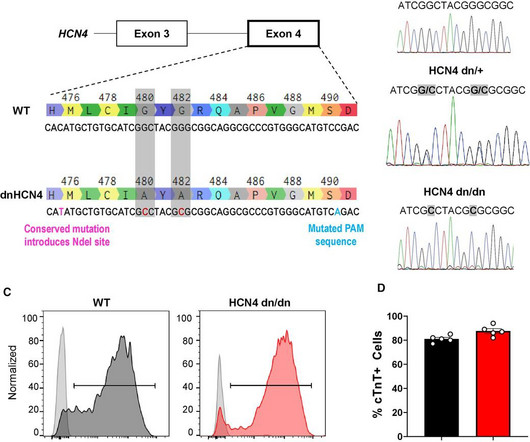
During early childhood, 50% of patients develop multifocal atrial tachycardia, a treatment-resistant tachyarrhythmia of unknown pathogenesis. HCN inhibitors targeted pacemaker-like activity in mutant ACMs. Circulation: Arrhythmia and Electrophysiology, Ahead of Print. Automated patch clamping assessed funny currents.
The researchers were able to show that those who had been ill with COVID-19 could also suffer from heart rhythm disturbances, both in the form of so-called tachycardias , when the heart ha rate is high, and bradyarrhythmias , when the heart is slow so that a pacemaker is sometimes needed.
Short-long-short (S-L-S) electrocardiographic cycle length patterns are associated with incidence of ventricular tachycardia (VT) and ventricular fibrillation (VF). It is also recognised that pacemakers can facilitate these cycle length sequences, and that the observation of these sequences can predict future VT/VF events.
Many patients with mild to moderately reduced left ventricular ejection fraction (LVEF) that require permanent pacemaker (PPM) implantation do not have a concurrent indication for implantable cardioverter-defibrillator (ICD) therapy. However, the risk of ventricular tachycardia/fibrillation (VT/VF) in this population is unknown.
Ivabradine is an anti-arrhythmic agent that reduces the heart rate through inhibition of the pacemaker current of the sinoatrial node. It has been used to treat both inappropriate sinus tachycardia and sinus tachycardia related to heart failure in children and adults.
This can initiate ventricular arrhythmias like polymorphic ventricular tachycardia (PMVT). Given the LV-RV offset of 40 msec, she would have received these two tightly coupled pacemaker spikes in an asynchronous mode, in this unfortunate instance during her T wave. Telemetry showed pacer spikes initiating PMVT.
Interpreting the waves and detecting abnormalities: Typically, the heart conducts electricity in a pathway starting in the sinoatrial node (SA), our heart’s “natural pacemaker”, located in the wall of the right atrium. Sinus tachycardia – sinus rhythm above 100 bpm is a sinus tachycardia.
It's a very "fun" ECG, with initial ectopic atrial tachycardia (negative P waves in inferior leads conducting 1:1 with the QRSs), followed by spontaneous resolution to sinus rhythm. What About the Tachycardia? Today's regular SVT rhythm could be an ectopic atrial tachycardia ( ATach ) — or an automatic junctional tachycardia.
EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport. It is hard to make out P waves but you can see them best in V2, and notches in the T waves in other leads - this is a sinus tachycardia with a very long PR interval indicating first degree block.
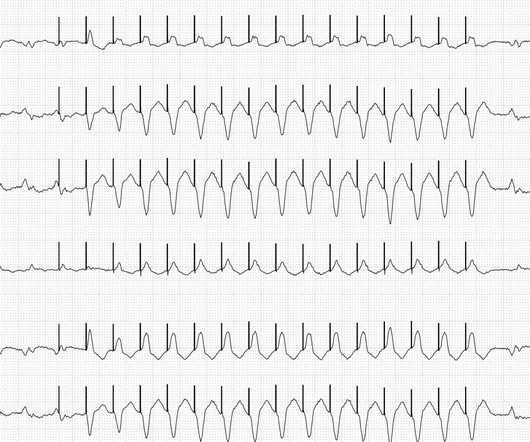
If ventricular tachycardia occurs in an ICD wearer, the ICD can combat this with 2 different forms of therapy, provided these are activated (which can be done using a programming device). First, the ICD attempts to overstimulate the tachycardia. Initially there is a relatively slow ventricular tachycardia with a heart rate of approx.
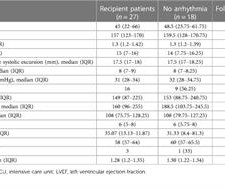
Three patients developed symptomatic sinus node dysfunction at 18, 25, and 38 days and received permanent pacemakers. One patient developed a complete AV block during acute rejection at 76 months and received a temporary pacemaker. One patient developed a complete right bundle branch block at 12 months.
An Initial ECG was performed: Initial ECG: Sinus tachycardia with prolonged QT interval (QTc of 534 ms by Bazett). She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
Multifocal Atrial Tachycardia 2. MAT has at least 3 distinct P-wave morphologies, but there is no single dominant pacemaker (i.e., P EARL # 4 — In “real life” — there is often NO distinct “cut-off” for differentiating between sinus tachycardia with multiple different-looking PACs vs MAT. Sinus with multifocal PACs 3.
Refers to: “PVC response Atrial-Pace,” an algorithm designed for preventing pacemaker-induced tachycardia after premature ventricular contractions, triggers atrial high rate episodes.1
Despite the scarcity of data, guidelines recommend ICD rather than a pacemaker implantation whenever a device is needed. Atrioventricular block (AVB) is a frequent initial presentation of cardiac sarcoidosis (CS), but dangerous ventricular arrhythmias (VA) can occur.
A 74-year-old man with a heterotopic heart transplant experienced alternating episodes of sustained native heart ventricular tachycardia and prolonged asystole. These were managed with cardioversion, drug therapy and pacemaker insertion.
1 A major limitation of an S-ICD is its inability to deliver anti-tachycardia pacing (ATP) for monomorphic ventricular tachycardia (MMVT). 2 Novel extravascular ICDs or modular device systems, which combine an S-ICD with a leadless pacemaker, offer the benefits of an S-ICD with the option for ATP.
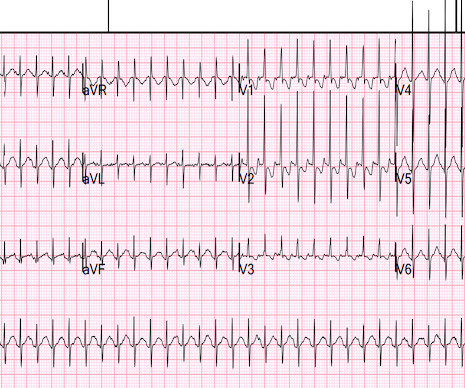
The ECG was done because the heart rate was 230 and the differential included SVT vs. sinus tachycardia. The computer read is usually very good at determining pacemakers and intervals, but it was way off in this case: it said: "electronic ventricular pacemaker" and measured the QRS at 202 ms!
While the initial impression might not immediately suggest ventricular tachycardia (VT), a closer examination raises suspicion. Again, see Ken's discussion below) Discussion continued The absence of pace spikes suggests this is not a pacemaker/ICD-related rhythm in this patient with an ICD. What is the rhythm? Smith : Are they P-waves?
Although sinus tachycardia is the most commonly encountered rhythmic disturbance, subsequent reports have highlighted other findings. Catheter-directed thrombolysis and a temporary pacemaker insertion were carried out sequentially. She presented with presyncope and an initial blood pressure of 77/63 mmHg.
The ECG and long lead II rhythm strip in Figure-1 — was obtained from a COVID positive patient with persistent tachycardia not responding to Diltiazem. Figure-1: The initial ECG — obtained from a patient with persistent tachycardia. ( MAT is not a Wandering Pacemaker. How would YOU interpret this tracing?
(Ken Grauer points out that this 5th beat appears to be due to an early atrial beat and that these early beats continue for a few beats, suggesting a short run of atrial tachycardia.) Our electrophysiologists give an example of this here: "Asynchronous" mode means that the pacemaker will pace regardless of what the native beats are doing.
Figure-2: We have labeled ECG #2 to explain the rhythm ( See text ). == Clinically — Brief appearance of a coronary sinus rhythm until a PAC reset the sinus pacemaker did not affect outcome in this case.
Among these were sinus node dysfunction in 14 patients (1.8%), AVB in 41 (5.2%), supraventricular tachycardia in 42 (5.3%), and ventricular tachycardia in 2 (0.3%). Subsequently, 8 patients underwent pacemaker implantation, 1 for sinus node dysfunction (post‐AF conversion pause of 9 seconds) and 7 for advanced AVB.
CRT is a type of pacemaker in which three chambers of the heart are paced, right atrium, right ventricle and left ventricle. The timing of the stimuli given by the pacemaker is adjusted to produce synchrony of contractions of the left ventricle. This picture illustrates what reduced ejection fraction means.
Secondary endpoints are 30 s or more persistent supraventricular tachycardia and ventricular tachycardia, 3 s or more persistent pause, bradycardia with 40 beats per minutes or lower heart rate, AF burden, all-cause death, cardiovascular death, hospital readmission due to exacerbation of HF, acute coronary syndrome, ischaemic or haemorrhagic stroke, (..)
We admitted him for probable EP study and possible pacemaker. He underwent pacemaker placement and is doing fine. SSS is by far the most common reason for permanent pacemaker placement. The indication for pacemaker placement with SSS is symptomatic bradycardia. Hyperkalemia might do this, but the K was normal.
This progressed to electrical storm , with incessant PolyMorphic Ventricular Tachycardia ( PMVT ) and recurrent episodes of Ventricular Fibrillation ( VFib ). If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing").
with one documented SP after termination of atrial tachycardia at the 3-month follow-up. Conclusion CNA may be an effective alternative to pacemaker implantation in pediatric patients with syncope or significant symptoms secondary to functional SP or AVB. Post-CNA, the median longest pause was 1.3 s s (range 0.8–2.2)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content