This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
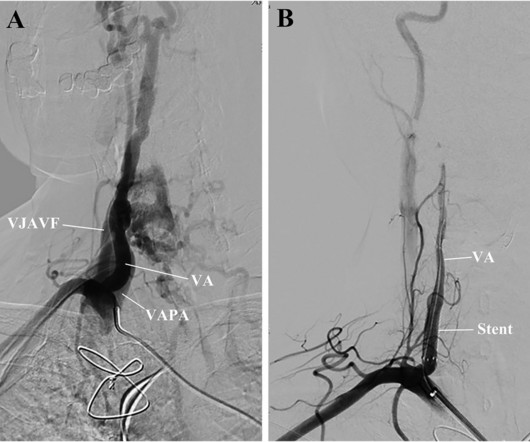
However, the symptoms persisted even after permanent pacemaker implantation and transcatheter closure of the aortic paravalvular leak. Using the endovascular technique, a 4mm stent graft was deployed in a 3.6mm VA to cover both the VJAVF and the VAPA ostia. The symptoms of dizziness disappeared.
An 80-year-old man with renal disease on hemodialysis, coronary artery disease, complete heart block and a dual chamber leadless pacemaker (LP) implanted because of previous bacteremia, presented with syncope. While in the hospital, he had witnessed ventricular fibrillation (VF) arrest for which he received external defibrillation.
Lead related venous obstruction (LRVO) is an often underrecognized complication of pacemaker implantation. We present an unusual case of a 54-year-old man with a history of retained pacemaker leads placed 26 years ago who presents with abdominal distention, lower extremity edema, and shortness of breath.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This was stented with a 2.25 x 38mm stent, post dilated with a 2.75mm balloon proximally.
She also has sick sinus syndrome (SSS) and intermittent high grade AV block for which she had a dual chamber pacemaker implanted. At that visit the patient was found to have an in-stent RCA occlusion. The patient was referred emergently to the cath lab, and again there was an in-stent RCA occlusion.
The documentary includes interviews with pioneers of interventional cardiac catheterization, in which multiple x-rays are used to navigate stents, valves, pacemakers and other devices through the vascular system and into and around the heart to restore patient health without resorting to the risks posed by open-heart surgery.
An epicardial pacemaker was implanted. The superior limb of the baffle was stenosed and required stenting. In 1973 she underwent a Mustard operation, switching atrial blood flow using a baffle, which was complicated by complete heart block. In 2012, she had a ventricular fibrillation cardiac arrest.
We describe a case of ventricular pacemaker spikes delivered on the T wave causing PMVT.Case:A 53-year-old female with CAD s/p stent, postpartum cardiomyopathy s/p Bi-V CRT-D (Boston Scientific G124), and paroxysmal atrial fibrillation presented for elective endoscopy and colonoscopy to evaluate her dysphagia and abdominal pain.
The patient is female in her 80s with a medical hx of previous MI with PCI and stent placement. She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. She also has a hx of paroxysmal atrial fibrillation and is on oral anticoagulant treatment. small squares in width (260ms).
She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. About 45 minutes after the second EKG, the patient was found in cardiac arrest. She was worked as a full code, and ROSC was achieved.
We offer a wide range of diagnostic and treatment services including: Coronary artery bypass surgery Angioplasty and stenting Heart valve surgery Pacemaker and defibrillator implantation Cardiac rehabilitation We believe every patient deserves personalized care.
And finally, after placement of a stent in the LAD: Before and after: (Unfortunately, this resulted in the "jailing" of the septal branches behind the stent and probably some degree of plaque shift which is why they do not opacify well in the "after" shot. This was the cost of preventing infarction of the anterior wall.)
He had previously undergone non‐contrasted head computed tomography (NCHCT) (magnetic resonance imaging (MRI) was unable to be performed secondary to pacemaker), which did not reveal strokes. Episodes always occurred after activity and only upon sitting. His initial computed tomography angiogram (CTA) of the head and neck was unremarkable.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
The patient was then taken to the cath lab an found to have a proximal RCA 100% thrombotic occlusion which was successfully stented. The transvenous pacemaker was removed the following day and pressors were not required again. Peak troponin T was 3.00 ng/mL (highly elevated). Post-cath ECG with resolution of acute changes.
He was rushed to the Cath Lab where an LAD culprit lesion was stented. Here is the LAD after stent placement. I initially suspected V2 as being placed too high on the chest, but there is no accompanying inverted P wave here, so the positioning is sound. It’s important to stress the presence of a normal QRS (i.e.,
Also a h/o LV aneurysm with thrombus, on anticoagulation, as well as a dual chamber pacemaker. It was opened and stented with resulting TIMI-3 (normal) flow. The stent to LCX is patent. She had a history of PCI to the circumflex and also of severe mitral regurgitation, status post bioprosthetic valve replacement.
Slow TIMI 2 initially with brisk flow status post percutaneous coronary intervention with 18mm drug-eluting stent. It is also not a wandering pacemaker — because change in atrial pacing site is gradual with that disorder. In the available view, the RCA appears fully occluded. To our knowledge, the patient did well.
Some patients with pacemakers and metal prosthesis can’t be exposed to such strong magnetic fields. It is a super specialised discipline. It requires very expensive machinery. It is inherently uncomfortable for the patient as you have to lie in a tight tunnel for up to an hour.
So in heart failure, one procedure that can help improve quality of life is the implantation of a biventricular pacemaker. It is worth knowing that people who may not have been deemed suitable for heart transplantation once upon a time may now be candidates because the laws around organ donation have changed.
These issues can only be addressed in an ICCU (Intensive Coronary Care Unit) setting, where temporary pacemakers and defibrillators are available. Then angioplasty is performed, and a medical device called a stent (metallic scaffold) is deployed in the artery to open the blood flow. This is known as a pharmaco-invasive approach.
All the patients had a history of catheter placement or pacemaker implantation. The characteristics of CVS and the clinical effectiveness of these procedures were evaluated.ResultsThis study included 26 hemodialysis patients who presented with symptomatic CVS. Of these 26 patients, 53.85% were male, and their mean age was approximately 54.96
After stent deployment, we often see improvement in the ST-T within seconds or minutes. Here is the final angiogram following placement of a stent in the ostial RCA. 2:04 PM, post stent deployment You can see that even after complete restoration of flow, the ECG still looks terrible, V most of all.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content