This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
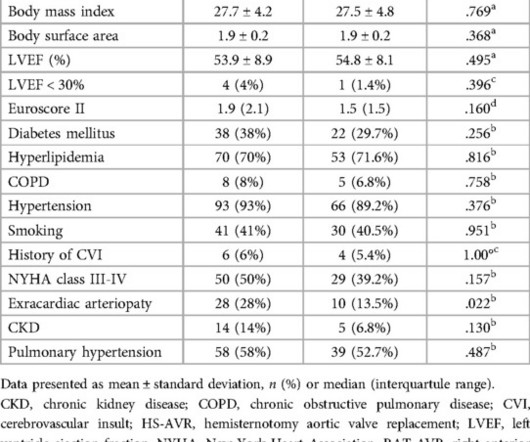
IntroductionSince TAVR was approved for lower-risk aortic stenosis (AS) patients, managing post-implantation conduction disturbances has become crucial, especially with self-expanding heart valves (SEV). Forty-seven received SEVs using COL, and 50 with CON techniques.
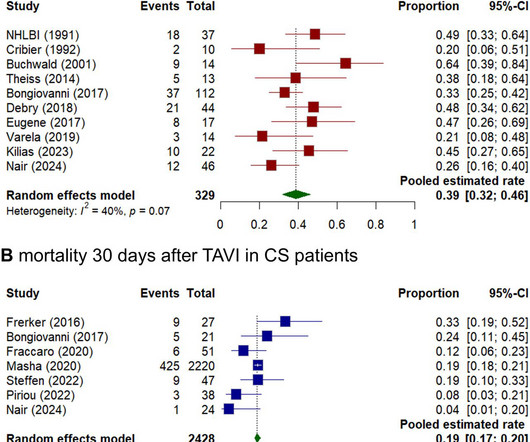
Background Cardiogenic shock (CS) induced by severe aortic stenosis (AS) is a life-threatening condition with high mortality. Despite advancements in emergency interventions, the optimal treatment approach remains uncertain. The primary endpoint was mortality at 30 days. Results Seventeen studies were included, totalling 2811 patients.
At 30-day follow-up, all-cause mortality, the incidence of major adverse cardiovascular events, major vascular complications, and new permanent pacemaker implantation were 3.8%, 4.6%, 0.8%, and 0.8%, respectively. Device and procedural success were achieved in 98.5% of the patients, respectively.
In this week's View, Dr. Eagle looks at secular trends of incidence and outcomes in severe aortic stenosis. He then examines titration of medications after acute heart failure.
In the meta-analysis of seven randomized trials, published in JSCAI and presented at the 2024 EuroPCR conference in Paris, France, researchers compared the outcomes of 7,785 patients undergoing TAVR (a procedure that delivers a new aortic valve into the heart through a catheter) to those undergoing SAVR for severe aortic stenosis.
Backgrounds Permanent pacemaker implantation (PPMI) is one of the greatest disadvantages of transcatheter aortic valve implantation (TAVI). Methods We retrospectively analysed data from 745 consecutive patients who underwent TAVI for severe aortic stenosis from November 2013 to July 2022. vs 9.1%±9.7%; p=0.035).
BACKGROUND:Current guidelines recommend surgical aortic valve replacement (SAVR) for patients with severe aortic stenosis and unfavorable iliofemoral access. In contrast, vascular complications and the need for permanent pacemaker implantation occurred more often in the TC-TAVR group (P=0.01 andP=0.001, respectively).
Due to atrial and ventricular pacing dependence, a comprehensive congenital care team concluded the need for lead extraction and replacement of pacemaker via leadless peacemaking device. Laser-lead extraction and temporary atrial pacemaker placement was performed.
In younger patients (<65 years), SAVR is recommended, as very few patients in this age group were enrolled in the randomized trials with additional concerns regarding transcatheter valve durability and higher rates of pacemaker implantation with TAVR.
BACKGROUND:Data concerning the outcomes of transcatheter aortic valve replacement in type 0 bicuspid aortic stenosis (AS) are scarce. Circulation: Cardiovascular Interventions, Ahead of Print. Ascending aortic diameter was the single predictor of 1-year mortality in type 0 bicuspid patients (hazard ratio, 1.59 [95% CI, 1.03–2.44];P=0.035).
Transcatheter aortic valve implantation (TAVI) has emerged as a safe and effective alternative to surgery in patients with symptomatic severe aortic stenosis, regardless of the baseline surgical risk.1,2
BACKGROUND:This study aimed to compare the incidence and prognostic implications of new-onset conduction disturbances after surgical aortic valve replacement (SAVR) in patients with bicuspid aortic valve (BAV) aortic stenosis (AS) versus patients with tricuspid aortic valve (TAV) AS (ie, BAV-AS and TAV-AS, respectively).
As ATTR-CM is associated with conduction disease, we sought to determine its prevalence in patients with idiopathic high-degree atrioventricular (AV) block requiring permanent pacemaker (PPM) implantation. All patients diagnosed with ATTR-CM had spinal canal stenosis and two had carpal tunnel syndrome.
They knew she would need a pacemaker unless some transient and reversible cause was discovered. Once this happens, of course, the patient will require temporary or permanent pacemaker as soon as possible. She required intermittent pacing from the temp wire numerous times overnight so a permanent pacemaker was placed the next day.
Transcatheter aortic valve replacement (TAVR) has increasingly become a safe, feasible, and widely accepted alternative surgical treatment for patients with severe symptomatic aortic stenosis.
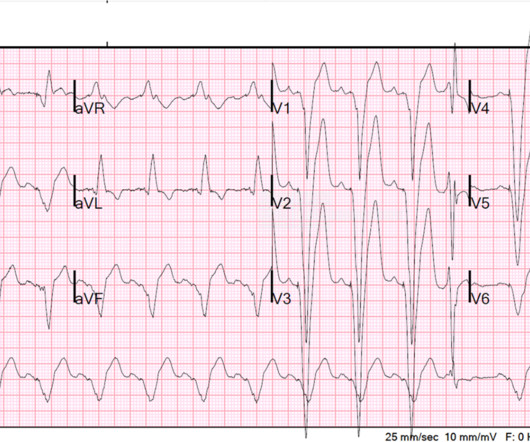
He presented with chest pain, not relieved by nitro, pain reproducible on exam and centered around the pacemaker insertion site. At that previous visit, he had had some mildly elevated troponins, but mostly had severe heart failure from very poor systolic function and aortic stenosis. Here is his ED ECG There is RV Pacing.
There were no statistically significant differences in terms of stroke, paravalvular leak, mechanical ventilation time, blood transfusion requirements, pacemaker implantation, reexploration for bleeding, conversion, wound infection, or in-hospital stay. This was a retrospective, single-center observational study.
He had previously undergone non‐contrasted head computed tomography (NCHCT) (magnetic resonance imaging (MRI) was unable to be performed secondary to pacemaker), which did not reveal strokes. Repeat CTA head and neck demonstrated multifocal intracranial atherosclerosis with marked stenosis of the left V4 segment.
Patients with bicuspid aortic valves (BAV) are predisposed to the development of aortic stenosis. to 0.63, p=0.01) but a higher risk of new permanent pacemaker placement (RR 2.17, 95%CI 1.03 Medical databases were queried to pool comparative studies of interest. There were 60,858 patients with BAV (7,565 TAVR, 53,293 SAVR) included.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chest pain associated with nausea/vomiting 30 min PTA. This was stented with a 2.25
Angiography : LMCA — 90-99% osteal stenosis. LCx — 50-69% stenosis of the 1st marginal branch; with 100% distal LCx occlusion. If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing").
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. So the patient was taken for emergent cath, showing: Culprit artery: LAD (100% stenosis, TIMI 0) requiring thrombectomy and stent.
The Y descent is shallow in tricuspid stenosis, and absent in cardiac tamponade. Thrombus can sometimes occur when there is a central venous catheter or a multiple pacemaker or defibrillator leads there that can cause thrombus formation. Right atrial hypertrophy as in tricuspid stenosis, pulmonary stenosis and pulmonary hypertension.
Also a h/o LV aneurysm with thrombus, on anticoagulation, as well as a dual chamber pacemaker. OM1 is occluded and OM2 has 60% stenosis. Her RCA is a medium caliber vessel with tandem, at least moderate stenosis in the mid segment. On arrival, the BP was 60/30. It was opened and stented with resulting TIMI-3 (normal) flow.
Cath report later that afternoon, around 25 hours since arrival: "There was a 70% proximal LAD stenosis secondary to a spontaneous coronary dissection with narrowing of the proximal LAD to at least 50% stenosis. Severe hypokinesis of the anteroseptal, anterior, inferoseptal, and apical myocardium. Normal RV function.
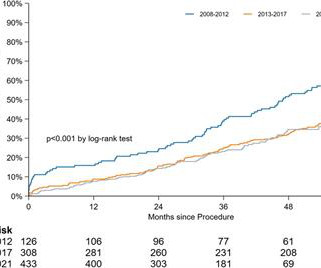
Background Treatment of severe aortic stenosis with transcatheter aortic valve implantation (TAVI) was introduced in 2002. As the incidence of most complications related to TAVI has decreased, the rates of permanent pacemaker implantation remain high.
Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. Negative predictors of adverse outcome: Pacemaker Pre-syncope or "near-syncope," but there is still some small risk (5, 18) These last two are identified in studies, but I consider them dangerous signs and symptoms in their own right, as above: 10.
(MedPage Today) -- The nitric oxide-independent soluble guanylate cyclase activator ataciguat continued to show promise for slowing the progression of fibrocalcific aortic valve stenosis in phase I and II studies. Circulation) The extent of myocardial.
Central vein stenosis (CVS) is a common vascular complication in undergoing hemodialysis, especially those with a history of catheterization. All the patients had a history of catheter placement or pacemaker implantation. However, the degree of venous stenosis in the PTS group was more severe than that in the PTA alone group.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content