This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Subtle as a STEMI." (i.e., A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. In our study, there were 20/53 complete LAD OMI (TIMI-0 flow) which did not meet STEMI criteria. None of the 20 ever evolved to STEMI criteria. This one is easy for the Queen.
He presented with chest pain, not relieved by nitro, pain reproducible on exam and centered around the pacemaker insertion site. is very specific for STEMI , and there is some evidence, as well as rationale, that a paced rhythm behaves similarly. Here is one case of anterior STEMI in a paced rhythm.
Three months prior to this presentation, he received a pacemaker for severe bradycardia and syncope due to sinus node dysfunction. His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”. This EKG seems to lack it.
In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. In other words, the inferior "ST elevation" is due to the abnormal rhythm, and does not signify OMI or STEMI in any way. This situation has been named "Emery phenomenon." YOU TOO CAN HAVE THE PM Cardio AI BOT!!
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. Most large STEMI have peak troponin I in the 20.0 She reports associated SOB but no dizziness or LOC.
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
Automatic activity refers to enhanced pacemaking function (typically from a non sinus node source), for example atrial tachycardia. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? The patient continued having chest pain. What is the rhythm? Moffat, M.
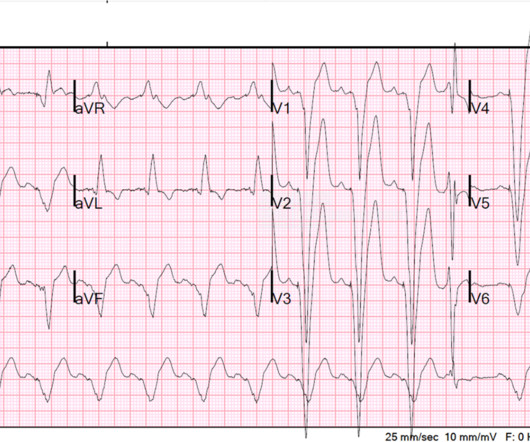
ST segments: There is obvious inferior STEMI, with ST elevation (and Q-waves and T-wave inversion) in II, III, aVF and reciprocal depression in I and aVL. or there is a low atrial pacemaker and 3rd degree block, and sinus brady, and junctional escape). Here is the initial ECG: Rhythm: slow and regular. What is it really?
There is STE in III and aVF which does not meet STEMI criteria due to insufficient STE in lead aVF. The interventionalists insisted that the ECGs did not meet STEMI criteria and cancelled the activation, stating that they would consider urgent cath after further stabilization. This is an obvious inferoposterior OMI.
The patient may need a pacemaker. CASE F ollow- U p: Providers in today's case recognized the above abnormalities — and promptly referred the patient to a PCI center for cardiac catheterization and potential pacemaker insertion. == L ooking C loser at Today's R hythm: The rhythm in Figure-1 has a number of complexities.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. If there had been — a temporary atrial pacemaker could have been considered as a way of increasing the heart rate to suppress a bradycardia-dependent arrhythmia ("overdrive pacing"). The below ECG was recorded.
Again, see Ken's discussion below) Discussion continued The absence of pace spikes suggests this is not a pacemaker/ICD-related rhythm in this patient with an ICD. Are the apparent P-waves (which now we suspect might not be P-waves) actually part of the QRS, in which case the QRS is even wider than it appears? Where does the QRS begin?
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chest pain: V5 and V6 sure look like a STEMI For this ECG and chest pain in the ED, the Cath lab activated. But the angiogram was clean. There was no OMI.
Is there STEMI? A Patient with Ischemic symptoms and a Biventricular Pacemaker Most physicians, at first glance, get this wrong. What is it? What is the rhythm? And is there new left bundle branch block (LBBB)? Is this Left Bundle Branch Block? Giant R-waves. What are they?
The medics recorded the following initial ECG at time 0: The computer read (see below) gives no further comment beyond ventricular pacemaker. And, in cases like the elderly patient with new-onset chest pain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. What do you think?
Anterior STEMI? This gradual change in P wave morphology as the heart rate varies could be consistent with a wandering atrial pacemaker. T-wave inversions and dynamic ST elevation Tachycardia, hyperthyroid, and ST elevation. What is it? 2 Cases of Resolved Chest Pain with Dynamic Terminal T-wave Inversion Is it Wellens' Syndrome?
A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center. It’s important to stress the presence of a normal QRS (i.e.,
Using the STEMI paradigm would have resulted in significant delays for this patient, which correspond with the doubled mortality and morbidity of NSTEMI Occlusions seen in over 50,000 subjects in NSTEMI trials. == MY Comment, by K EN G RAUER, MD ( 9/30/2019 ): == Our THANKS to Dr. I never see 2 P waves in a row with the same morphology.
100% occluded RCA with TIMI 0 flow Post drug-eluting stent placement with TIMI 3 flow While in the cath lab, she transiently developed complete heart block and became hypotensive requiring transvenous pacemaker placement and transient pressors. The transvenous pacemaker was removed the following day and pressors were not required again.
In fact, sometimes the sinus node is working and acting as a pacemaker but no P waves are visible!! See many examples of Pseudo STEMI due to hyperkalemia at these two posts: Acute respiratory distress: Correct interpretation of the initial and serial ECG findings, with aggressive management, might have saved his life.
Learning Points: Ectopic atrial rhythm can produce atrial repolarization findings that can be confused for acute ischemia, STEMI, or OMI. The patient was worked up for abdominal pain with unclear diagnosis, and he was able to be discharged.
Also a h/o LV aneurysm with thrombus, on anticoagulation, as well as a dual chamber pacemaker. Marked acute STEMI changes in no less than 4 lateral leads. She had a history of PCI to the circumflex and also of severe mitral regurgitation, status post bioprosthetic valve replacement. On arrival, the BP was 60/30.
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." As the troponin T was 1521 ng/L (peak troponin T over 1000 ng/L is typical of STEMI) and still rising, no further troponins were measured. NOTE #2: I always like to look for the presence of an underlying rhythm in pacemaker tracings.
Abnormal ST elevation is also seen in the high-lateral limb leads ( = leads I and aVL ) which together with the abnormal ( and very large ) Q waves and QS complexes in 8/12 leads suggests that the reason for this ventricular rhythm is a recent and/or ongoing extensive antero-lateral STEMI. The above said Today's patient had other ideas.
2:34 PM, following right heart catheterization She then went into atrial fibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker. There was indication of parasympathetic overdrive ( the acute inferior STEMI with profound bradycardia and junctional escape ).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content