This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Lead related venous obstruction (LRVO) is an often underrecognized complication of pacemaker implantation. We present an unusual case of a 54-year-old man with a history of retained pacemaker leads placed 26 years ago who presents with abdominal distention, lower extremity edema, and shortness of breath.
Welcome to the Physiology Friday newsletter. Physiologically Speaking is a reader-supported publication. To assess the impact of light on circadian rhythms, a model of the human circadian pacemaker was used, simulating how light exposure affects circadian amplitude and phase—two critical components of a healthy internal clock.
In ambulatory patients with complete heart block (CHB), dual-chamber (DDD) pacing confers physiological benefits versus single-chamber (VVI) pacing, however, the impact on mortality is disputed. In nonagenarians with emergent CHB, we compared the clinical characteristics and outcomes of patients receiving VVI versus DDD pacemakers.
Abstract Introduction Clinical outcomes of long-term ventricular septal pacing (VSP) without His-Purkinje capture remain unknown. This study evaluated the differences in clinical outcomes between conduction system pacing (CSP), VSP, and right ventricular pacing (RVP).
Introduction Amyloid light-chain cardiac amyloidosis is a progressive infiltrative disease characterized by the deposition of amyloid fibrils in the cardiac tissue, which can cause serious atrioventricular block requiring pacemaker implantation. Left bundle branch pacing was performed successfully.
In patients undergoing non-physiologicpacemaker (PM) implantation (eg, RV pacing), cardiomyopathy (CM) may develop - particularly in patients with an elevated pacing burden.
Interpreting the waves and detecting abnormalities: Typically, the heart conducts electricity in a pathway starting in the sinoatrial node (SA), our heart’s “natural pacemaker”, located in the wall of the right atrium. This allows the atria to fill the ventricles and achieve the highest possible stroke volume.
Left bundle branch area pacing (LBBAP) can deliver near physiological electrical activation of the heart, but reliability and stability of this approach remains unclear.
Conduction system pacing, namely His bundle and left bundle branch area (LBBA) pacing, has emerged as a promising modality to maintain physiologic conduction with ventricular pacing in several scenarios, providing patients with electrical and mechanical synchrony.
These were managed with cardioversion, drug therapy and pacemaker insertion. The unique physiology in such patients lends itself to numerous clinical considerations that would otherwise be routine management for most.
Left bundle branch pacing (LBBP) has proven to be an alternative method for delivering physiological pacing to achieve electrical synchrony of the left ventricle (LV), especially in patients with atrioventricular block and left bundle branch block (LBBB). Approximately 2%–12% of patients may need pacemaker implanted after Morrow surgery.
Atrioventricular nodal (AVN) ablation with permanent pacemaker implantation – ‘pace and ablate’ – may be considered for patients with symptomatic atrial fibrillation (AF) for whom rhythm control has been unsuccessful. This creates concerns about inducing pacemaker dependence and potential pacemaker-induced cardiomyopathy (PICM).
Asynchronous pacing seems like the safe setting, EXCEPT that it means that the pacemaker can trigger on the T-wave, which can result in Ventricular Fibrillation. Our electrophysiologists give an example of this here: "Asynchronous" mode means that the pacemaker will pace regardless of what the native beats are doing.
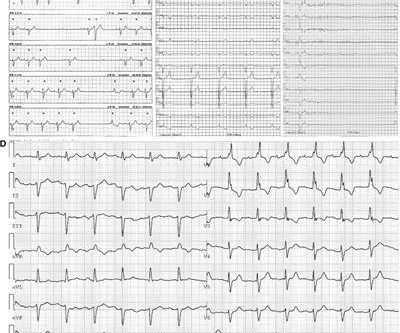
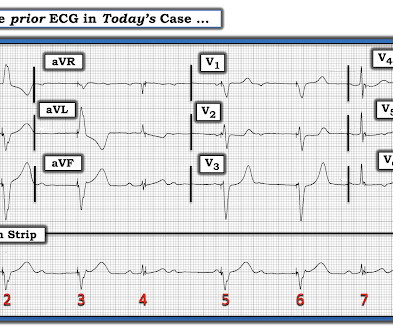
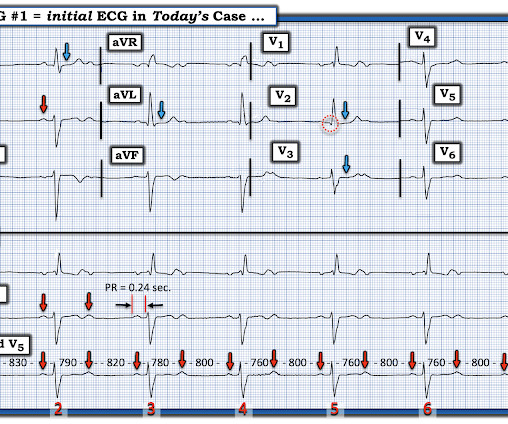
At the time this Old ECG was done — the patient had a pacemaker. Is the pacemaker functioning appropriately? ie, WHY do you think the pacemaker was needed? ). It is no longer easy ( or even possible ) to fully assess pacemaker function solely from the ECG without knowledge of pacing specifications for that particular patient.
The depolarization phase of pacemaker cells is mainly due to L-type calcium channels (ICa-L) There is some contribution to the diastolic depolarization phase by T type calcium channels (ICa-T). The physiological and pharmacological significance of cardiovascular T-type, voltage-gated calcium channels. References Triggle DJ.
She had a single chamber ICD/Pacemaker implanted several years prior due to ventricular tachycardia. Seeing as the patient has a single chamber ICD/pacemaker, pacing the ventricle will also lead to AV dyssynchrony that will compromise ventricular filling, further impairing hemodynamics. small squares in width (260ms).
It was first described over 150 years ago, however the physiological mechanism and pathophysiological implications are not well understood. This study aimed to elucidate underlying mechanisms and physiological function of vasomotion in human arteries.
ABSTRACT Background Left bundle branch pacing (LBBP) emerged as a novel physiological pacing modality that improves clinical outcomes. Left bundle branch pacing (LBBP) significantly increased X- and Y-axis RWA independent of pacing voltage in both CLBBB and narrow QRS patients.
In addition, we have identified 2 cardiomyocyte‐like conducting cells, lending support to the theory that the sinoatrial node pacemaker cells are specialized cardiomyocytes.
CRT, a pacemaker that corrects abnormal electrical conduction by simultaneously pacing the left and right heart chambers, is a well-established therapy for improving cardiac efficiency. Approximately 6.7 million adults in the U.S. have heart failure, and the prevalence is expected to rise to 8.5 million by 2030.
Isoprenalin was discontinued, and a temporary transveous pacemaker was implanted. The patient stabilized following pacemaker placement. The physiologic reason for this — is thought to be the result of momentarily increased circulation from mechanical contraction arising from the "sandwiched in" QRS complex.
Among 299 patients with CRT-pacemakers (BVP-111, LBBAP-188), VT/VF occurred in 8 patients in the BVP group vs. none in the LBBAP group (7.2% Physiologic resynchronization by LBBAP may be associated with lower risk of arrhythmias compared with BVP. The occurrence of VT/VF was significantly lower with LBBAP compared with BVP (4.2%
It is a physiological adaptation helping athletes perform physical tasks better than non-athletes. Though sinus bradycardia is usual, other abnormalities like sinus arrhythmia, sinus arrest, wandering atrial pacemaker and coronary sinus rhythm have been described. References 1.Prior Prior DL et al. The athlete’s heart. Athlete’s heart.
The aim of CRT is to restore physiologically normal electrical heart activity, which is often altered in the course of the underlying disease. This can be achieved by introducing electrodes into the vascular system which are connected to a pacemaker with a resynchronization function.
It is also unique because it works using the Doppler effect, you can get not only an anatomical evaluation of the heart but also physiological assessment. Some patients with pacemakers and metal prosthesis can’t be exposed to such strong magnetic fields. An echo is easy to do, risk free and easily accessible.
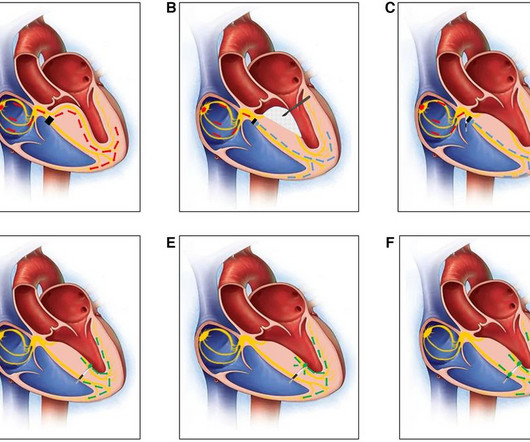
Because of the complexity of pacemaker troubleshooting — I was happy to find the wonderful on-line “primer” ( with color-coded illustrations ) by Dr. Harry Mond — that outlines a user-friendly approach to — “Where Am I Pacing From?” NOTE #2: I always like to look for the presence of an underlying rhythm in pacemaker tracings.
Negative predictors of adverse outcome: Pacemaker Pre-syncope or "near-syncope," but there is still some small risk (5, 18) These last two are identified in studies, but I consider them dangerous signs and symptoms in their own right, as above: 10. QRS Syncope with Exertion (EGSYS) 7. S yncope while supine (EGSYS) 8. orthostatic vitals b.
More than 1 million permanent pacemakers are implanted worldwide each year, half of which are in patients with high-grade atrioventricular block. Pacemakers provide adequate frequency support in the initial stage, but traditional right ventricular (RV) pacing may lead to or aggravate left ventricular dysfunction and arrhythmia.
How does a pacemaker accomplish RBBB morphology? Quick aside on device terminology (feel free to skip): A "single chamber" pacemaker is a device with only one lead. A "dual chamber" pacemaker is a device with an atrial lead and a ventricular lead. By ignoring this, the pacemaker reduces the likelihood of PMT.
A permanent pacemaker was placed and the patient was atrial paced at 60bpm. After pacemaker placement — a ß-blocker was initiated. Learning points : Dual AV physiology in the retrograde direction does not necessarily mean there is dual AV conduction in the antegrade direction. Figure-7: I've labeled Figure-6.
If there is PR prolongation from one to the next, this supports Mobitz I physiology which rarely benefits from pacing. Conversely, if the PR interval is constant , this supports Mobitz II physiology, which is an indication for pacing. This pattern can be seen in both Mobitz I and Mobitz II physiology. History is often helpful.
2:34 PM, following right heart catheterization She then went into atrial fibrillation with complete heart block and junctional escape rhythm prompting placement of transvenous pacemaker. Clearly the physiologic chain reaction of autonomic dysfunction seen in todays case does not commonly lead to death of the person learning this news.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content