This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
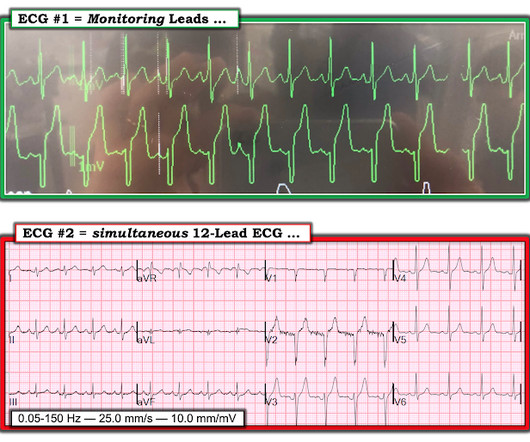
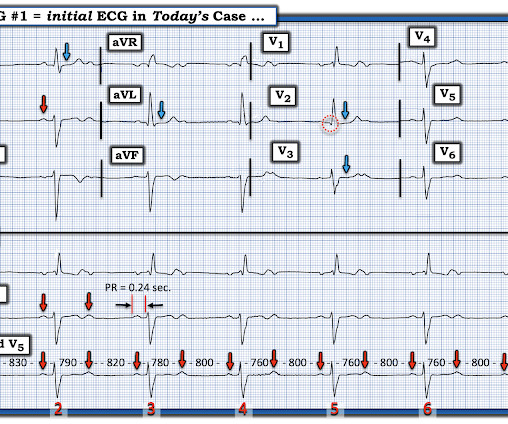
Written by Willy Frick A man in his 70s with a history of HFrEF and sick sinus syndrome s/p dual chamber pacemaker placement was admitted for overnight observation following outpatient placement of a mitral valve clip. This is unambiguous evidence of pacemaker malfunction. Imagine the pacemaker is set at a minimum rate of 60.
Select procedures performed outside the hospital setting—such as diagnostic cardiac catheterization, non-acute percutaneous coronary interventions and defibrillator and pacemaker implantations—closely intersect with existing data collection occurring in the NCDR CathPCI Registry and EP Device Implant Registry.
Place temporary pacemaker 3. Discontinue all negative chronotropic agents, since the risk of torsade is much higher with bradycardia or pauses. See this post: How a pause can cause cardiac arrest 2. Discontinue amiodarone, since it prolongs the QT 4. Discontinue all QT proloning medications, including azithromycin 6.
They knew she would need a pacemaker unless some transient and reversible cause was discovered. Once this happens, of course, the patient will require temporary or permanent pacemaker as soon as possible. She required intermittent pacing from the temp wire numerous times overnight so a permanent pacemaker was placed the next day.
Hopefully his outpatient EP appointment will understand and correct that. No use of drugs, stimulants, etc. was discovered. Unfortunately the patient was erroneously diagnosed with "SVT / atrial fibrillation" and put on apixaban!!! See more posts on the atrial repolarization wave: K.
He was discharged and schedule for an outpatient echo which has not been done yet. A Patient with Ischemic symptoms and a Biventricular Pacemaker : ) Ken Case Outcome: The patient had never had any cardiopulmonary complaints, was otherwise completely healthy. He was admitted overnight and had no complications. Is there STEMI?
Written by Willy Frick A middle aged man presented for elective outpatient surgery. The patient went for EP study and had prolonged HV interval which strongly supports placement of a pacemaker. He underwent dual chamber pacemaker implantation and did well. The following ECG was obtained in the preoperative area.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content