This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Transcatheter aortic valve replacement (TAVR) is the standard treatment for severe aortic stenosis, but post-TAVR leaflet thrombus, identified by hypoattenuated leaflet thickening (HALT), poses potential risks like cerebral thromboembolic events. Perivalvular thrombus has also been reported. had thrombus at any aortic valve complex.
Some of the late-breaking topics that will be covered include transcatheter aortic valve replacement (TAVR), peripheral artery disease (PAD), and pulmonary embolism (PE): Impact of Age on Procedural Timing for Asymptomatic Severe Aortic Stenosis: Results from the Early TAVR Trial The PERFORMANCE II Trial: A Prospective Multicenter Single Arm Investigation (..)
Stroke, Volume 56, Issue Suppl_1 , Page ADP36-ADP36, February 1, 2025. All patients had headache, and funduscopic examination demonstrated papilledema for all patients. All patients had headache, and funduscopic examination demonstrated papilledema for all patients. Additional randomized and controlled clinical research is deserved.
The stenosis was treated with a stent. years later he presented with an in-stent restenosis that was successfully treated with a stent-in-stent strategy. Conclusion Our case demonstrates stenting as a viable alternative strategy with potentiallyfavorable long-term outcome.
Stent performance was assessed.ResultsWe identified 28 patients (67.8% Percentage of stenosis was 50% (IQR, 36%58%). The procedures mostly used 7 Fr sheaths for stents on 6, 7, and 8 mm balloons and 8 Fr sheaths for 9, 10, 12 mm balloons. Median stent expansion percentage was 95% (IQR, 90%96%). kg (IQR, 9.116.4).
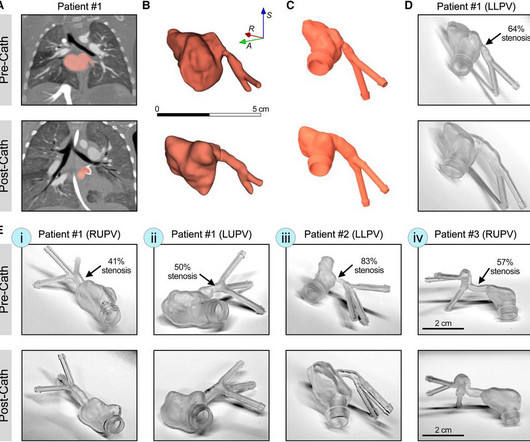
IntroductionPrimary pulmonary vein stenosis (PVS) is a rare congenital heart disease that proves to be a clinical challenge due to the rapidly progressive disease course and high rates of treatment complications.
Initial suspicion of underlying ICAD could help in the early adoption of rescue techniques, reducing the total number of passes and increasing the chances of sustained final recanalization and favorable outcomes. Bailout strategies were required more often in the IS+ group (34.6% Vs12.8%; p=0.001), and procedural times were longer (56.6
Introduction:Medical therapy and endovascular therapy for intracranial atherosclerotic disease (ICAD) have evolved over the past two decades with improved medical therapy benchmarks, and improved techniques and patient selection for stenting. There were significantly higher incidences in uncontrolled hypertension (28.2%
The red arrow shows a roughly 80% stenosis of the proximal LAD. The blue arrow shows another stenosis of the LAD distal to the first diagonal branch of about 99%. The green arrow shows a 95% stenosis of the ostium of the first diagonal branch. All three lesions had TIMI 2 flow prior to stenting.
BACKGROUND:Carotid artery stenting (CAS) is an alternative treatment for patients with carotid artery stenosis who are not eligible for carotid endarterectomy. The primary outcome was a composite of ischemic stroke, gastrointestinal bleeding, and intracranial hemorrhage within 12 months of switching to single antiplatelet therapy.
Rescue treatment with stenting, balloon angioplasty, and/or intraarterial thrombolysis or antiplatelets are often required to treat the underlying stenosis. 4 Recent literature has reported clinical benefits associated with rescue stenting in the setting of ICAD‐related MT‐refractory strokes.5
We defined high-risk post-EVT stenosis as any stenosis with 50% lumen stenosis, associated dissection, re-occlusion during thrombectomy, and severe residual luminal irregularity. Conclusions:Eptifibatide use is associated with lower re-occlusion rates in patients with residual high-risk stenosis after EVT.
IntroductionVertebral artery stenting represents a viable option in treating symptomatic vertebral artery atherosclerotic stenosis. We included articles reporting patients > 18 years old with symptomatic extracranial vertebral artery stenoses due to atherosclerosis treated with stenting (with or without angioplasty).
OBJECTIVECarotid artery stenting for heavily calcified lesions is challenging for interventionists. A calcium burden is associated with suboptimal dilatation, periprocedural complications, high rates of restenosis, and poor outcomes. After postdilatation, the stenosis rates decreased to 21% and 23%, respectively.
In this hyperacute emergent clinical situation, covered stents have been considered as a primary measure to prevent further serious arterial events. A fabric-based covered graft stents yield poor clinical outcomes. Future human studies are warranted to validate these findings and elucidate the clinical outcomes of the study.
Background:Postoperative complication rates of carotid endarterectomy (CEA) and carotid artery stenting (CAS) for carotid artery stenosis are recommended to be maintained below a certain threshold. This study indicates the importance of considering surgical volume as a factor to improve outcomes of CEA and CAS in Japan.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This was stented with a 2.25 x 38mm stent, post dilated with a 2.75mm balloon proximally.
1, 2)These patients are also more likely to experience poor functional outcomes. (3) 3) Rescue stenting (RS) in these patients has shown promising rates of recanalization and better outcomes in preliminary studies. Therefore, rescue stenting can be considered as a safe and viable option in these patients.
BACKGROUND:In patients with post-thrombotic syndrome, stent recanalization of iliofemoral veins or the inferior vena cava can restore venous patency and improve functional outcomes. The risk of stent thrombosis is particularly increased during the first 6 months after intervention. points (P=0.36), respectively.
Background:Persistent hypotension after carotid artery stenting (CAS) can lead to adverse outcomes, prolong length of stay (LOS), and increase hospital costs. A relation between decline of norepinephrine after stenting and persistent hypotension supports the role of catecholamine in BP control.
Background:Hemodynamic evaluation is crucial in assessing stroke risk in patients with symptomatic intracranial atherosclerotic stenosis (sICAS). The primary outcome was a composite of recurrent ischemic stroke or TIA within the same arterial territory over one year.Results:In the first study, involving 22 patients (median age = 53 years, 81.8%
We compared demographics, radiological findings, clinical outcomes, and follow-up results between mismatch and no mismatch groups.Results:Among 73 patients, 20 (27.4%) had DWI-ADC mismatch. Follow-up lesion volumes and functional outcomes were similar; however, the mismatch group showed a slower infarct growth rate (3.8 ml/h vs. 7.5
Background:Hyperperfusion phenomenon (HPP) constitutes a significant risk factor for adverse outcomes following carotid artery stenting (CAS). Stroke, Volume 56, Issue Suppl_1 , Page ATP178-ATP178, February 1, 2025. Currently, the sole method for evaluating the risk of HPP post-CAS is the invasive acetazolamide (ACZ) challenge test.
Available from: [link] In this study, the major outcomes were the same for both groups, but of 70 patients in the delayed group, 4 required emergent intervention for sudden re-occlusion. Here are other very interesting posts: Wellens' syndrome: to stent or not? Eur Heart J [Internet]. 2019;40:283–291.
Background:Vertebrobasilar artery stenosis (VBAS) can cause posterior circulation strokes (PCS). Optimal management is controversial, with options including medical therapy (MT), endovascular stenting (ES), and surgical revascularization (SR). Circulation, Volume 150, Issue Suppl_1 , Page A4135852-A4135852, November 12, 2024.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. Does this change your interpretation?
Introduction:Current guidelines do not support the use of stenting for severe symptomatic intracranial atherosclerotic disease (ICAD) over maximal medical therapy (MMT) as first line treatment. Periprocedural stroke was defined as <7d from stent placement.
In this study, we evaluate the safety and efficacy of TCAR in patients with symptomatic internal carotid artery disease compared with carotid endarterectomy (CEA) and carotid artery stenting (CAS).METHODS:A The primary outcomes included a 30-day stroke or transient ischemic attack, myocardial infarction, and mortality.
We also compared the safety of acute carotid stenting (CAS) in TLs with low ASPECTS.Methods:This prospective multicenter study from 16 centers included patients with anterior circulation TL from 2015-2020. in patients with stenting (18/44) versus no-stenting (25/44).Conclusion:This 3.05; p=0.32), PH2 (OR: 1.14, CI: 0.26-5.02;
The primary outcomes included 30-day combined stroke and transient ischemic attack (TIA), myocardial infarction (MI), and mortality. Conclusions:Although CEA has traditionally been considered superior to stenting for symptomatic carotid stenosis, TCAR may have some advantages over CAS, particularly in the elderly population (≥80 years).
Treatment of ICAS‐LVO with rescue stenting and/or angioplasty has shown promising outcomes, but diagnosing ICAS‐LVO during MT can be challenging [2, 3]. Most neurointerventionalists (91%) diagnose ICAS‐LVO after a continued or recurrent occlusion or by the presence of fixed focal stenosis (FFS) after multiple MT attempts.
The PREMIER study first demonstrated high rates of complete occlusion without parent vessel stenosis or permanent neurological complications after the treatment of wide-necked small and medium-sized intracranial ICA aneurysms with the 48-wire pipeline. At a median 10.1 months (IQR: 6.3-12.6),
MRA head demonstrated multifocal arterial stenosis. Repeat CTA head/neck and CT perfusion showed severe stenosis of bilateral M1 segments and left greater than right A1 segments as well as ischemic penumbra in left ACA/MCA watershed territory. She was discharged home on HD20.ConclusionWe
The left circumflex had 80% proximal stenosis with minimal luminal irregularities in the mid to distal portion. After guidewire crossing, balloon angioplasty was performed, and a drug-eluting stent was deployed. An intravascular ultrasound was also performed, which was negative for vessel dissection.
Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer: This is a posterolateral MI. It was opened and stented. LM: No significant stenosis. LAD: luminal irregularities with a 40% stenosis at the take-off of a D3. D3 has a 95% tubular ostial stenosis.
Here is the angiogram: --Culprit is 100% stenosis in the proximal RCA. (It It must have re-occluded between the ED and the cath lab) --Lesion was stented. Thus, in our ECG research, we need to find a surrogate outcome that reflects the state of the artery at the time of the ECG.
CT angiography (CTA) showed near occlusive stenosis of the left carotid bulb with an acute thrombus within Supraclinoid Internal Carotid Artery (ICA) extending into the Left MCA and origin of Left Anterior Cerebral Artery (ACA). He underwent single pass complete recanalization, TICI 2C using Stent retriever and aspiration.
1,2 The National Institute of Health Stroke Scale (NIHSS) cutoff for poor outcomes is lower in BAO compared to anterior circulation large vessel occlusions (LVO) due to the scale’s weighted scoring towards cortical signs.3,4 3,4 To bridge this gap, Alemseged et.al 3,4 To bridge this gap, Alemseged et.al CT perfusion was without mismatch.
The red arrow points to a 90% stenosis in the proximal segment of the LAD. RAO Caudal View Post PCI This is the RAO Caudal view after thrombectomy and stent placement. Nevertheless, cases like the one presented today — illustrate the continued need for review of these points that are KEY to attaining a good outcome.
A stent was placed. I have seen cases of Wellens' syndrome that were ignored because of either negative troponins or normal echo or both and the patient did not get an angiogram and had a bad outcome. Wellen's syndrome is a Reperfusion syndrome. Am Heart J (1989) 117 : pp 657-665. de Zwaan C., Wellens H.J.J., Doevendans P.A.,
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The patient underwent successful placement of one drug eluting stent with restoration of TIMI 3 flow.
It was stented. Also, anterior MI could result from 1) ACS, but also from 2) severe ischemia due to combination of a hemodynamically significant LAD stenosis + severe hypotension during cardiac arrest. Here is the post cath ECG T-wave inversions consistent with anterior MI, but not diagnostic. The troponin I peaked at 8.1.
Angiogram showed a critical LAD thrombotic stenosis. The patient went to cath and had a distal LAD 99% stenosis with thrombus and TIMI-2 flow. After many hours, the decided that it was appropriate to do an angiogram and they found a distal LAD occlusion which was opened and stented. Outcome : The third troponin I, drawn 4.5
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. More outcome Peak troponin I was 0.58 Wellens' original Papers : de Zwaan C, Bär FW, Wellens HJ. Am Heart J. 1982 Apr;103(4 Pt 2):730-6.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content