This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
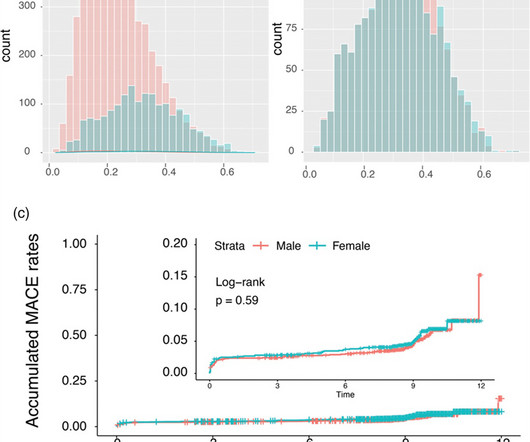
Background: Gender-specific outcomes after percutaneous coronary interventions were studied by a number of research groups with different endpoints and cohorts of different ethnic extractions. In the unmatched STEMI subgroup, all-cause mortality was significantly higher in females driven by older age (P < 0.001). vs. 3.9%; P = 0.020).
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion.
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardial infarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients. 3.45) and 4.47 (95% CI: 2.54–7.87),
This systematic review of the literature aims to explore outcomes in the patients treated with conservative management vs. invasive strategy. with ST elevated myocardial infarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. Approximately 48.5%
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. Most large STEMI have peak troponin I in the 20.0 This was stented with a 2.25 Next trop in AM.
. #5: 18 minutes after #4: STE is resolved #6: 4 minutes after #5: And remains resolved Case Outcome Because of ST resolution, the patient was not taken that night to the cath lab. Waiting to cath a transient STEMI can be hazardous. See this case in which I made that mistake.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. An open 90% LAD was stented.
As a low-volume PCI centre in the Middle East, we wanted to find out if the outcomes of our PCI procedures are different from those of high-volume PCI centres in the UK and the Western world. and the average number of stents 2.6. Prospectively collected data of all comers for PCI (urgent and elective) were retrospectively analysed.
Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." He diagnosed anterior "STEMI" and activated the cath lab. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? This was stented. The patient stabilized and had a good outcome. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 The patient stabilized. mEq/L: The STE is resolved.
Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. It must have re-occluded between the ED and the cath lab) --Lesion was stented. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.)
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
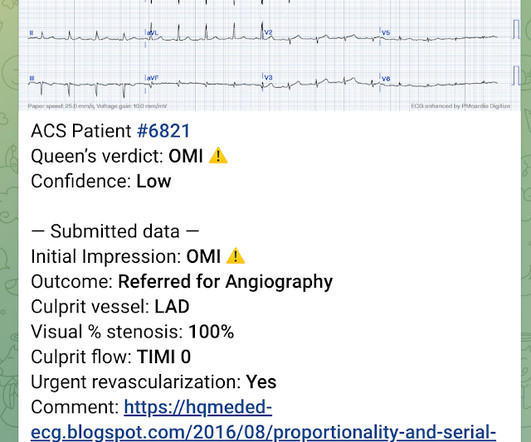
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Here is the angiogram after stent placement. Immediate versus delayed invasive intervention for non-stemi patients. Marinkovic, J.,
This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria. You can find the variables used to calculate the value on MD calc here: [link] Utilizing Dr. Smith’s Subtle Anterior STEMI Calculator (4-Variable), the value is greater than 18.2 The culprit mid LAD lesion was stented.
The cath lab was activated, and then not cancelled, and the angiogram showed 99% TIMI 2 flow proximal LAD culprit lesion, stented in less than 90 minutes of arrival. Outcome of case 2? Cath days later showed complete occlusion of the LAD, stented. Another missed OMI by the False STEMI-NonSTEMI Dichotomy Don't miss them!!!
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. I sent it to 5 of my OMI friends without any clinical information or outcome and all 5 independently responded with exactly the same diagnosis: "reperfused inferior OMI".
A meta-analysis was performed on primary outcomes of major adverse cardiac events (MACE) and all-cause mortality. A meta-analysis was performed on primary outcomes of major adverse cardiac events (MACE) and all-cause mortality. vs 13.6%), any stent thrombosis (RR=1.42; 95% CI [0.35, 5.72]; p=0.62; 2.2%
RBBB in acute STEMI has a very high mortality. A stent was placed, and the patient had an excellent outcome with no wall motion abnormality. Thus, there is right bundle branch block, which should never (unlike Left BBB) have any ST elevation. But here there is a large degree of ST elevation in V2-V6, I, and aVL.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
A male in late middle age with a history of RCA stent 8 years prior complained of chest pain. It is highly associated with proximal LAD occlusion and bad outcomes. Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiac arrest with unrecognized STEMI, died. New RBBB + LAFB is a very bad sign.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. So there is pathologic ST elevation here, consistent with anterolateral STEMI. Called 911.
Just as hyperacute T-waves can be reciprocal to T-wave inversion ( last case ),T-wave inversion can be reciprocal to STEMI of opposite wall! Outcome : She ruled in for MI by troponins and went for angiogram. An 80% thrombotic RCA was stented. This case was sent by Arthur Lee.
Inflammatory indicators such as neutrophil count and monocyte count potentially may predict patients’ outcomes and prognosis in ACS. Types of ACS include stable angina 5.3% (n=8), unstable angina 24% (n=36), NSTEMI 28.7% (n=43), and STEMI 24% (n=36). All patients had interventional PCI with balloon and stent insertion.
There is an obvious inferior posterior STEMI(+) OMI. Angiogram: Culprit Lesion (s): Thrombotic occlusion of the proximal RCA -- stented. Results Of 149 patients with inferior STEMI , 43 (29%) had RVMI and 106 (71%) did not. What is the atrial activity? Is it sinus arrest with junctional escape? How would one tell?
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 It was stented. This T-wave inversion morphology is very specific for Wellens' waves. Gottlieb SO, et al.
Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer: This is a posterolateral MI. It was opened and stented. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI.
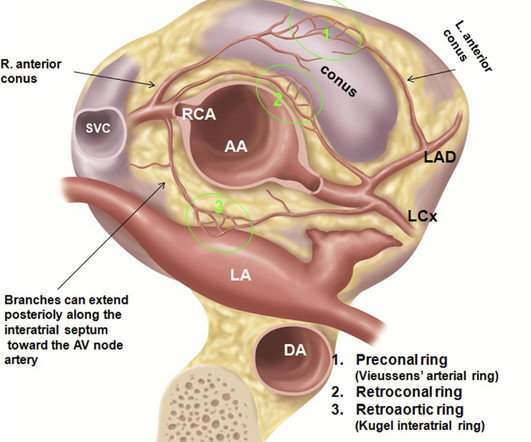
Final message Coronary arterial anomaly is a less discussed topic nowadays, unless & until, it intrudes an interventional cardiologist in his daily routine life, of delivering stents. We know, how adverse is the outcome of Left main STEMI. In reality, there could be thousands of asymptomatic ones in the public domain.
He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. No appreciable skin pallor. Is this OMI?
The paramedic interpreted this as a STEMI. Can you employ the Subtle Anterior STEMI calculator ? The Subtle STEMI calculation is used to differentiate a subtle anterior acute coronary occlusion from early repolarization (ER). [link] Two doses of nitroglycerin reduced the patient’s symptoms during transport. or LAD occlusion?
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Yet this is rarely followed, and patient outcomes like this are the result once in a while. Am J Emerg Med. 2014;32:e5–e8.
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. As a result, this 45-year old man did not experince any delay in treatment — and a large diagonal branch of the LAD was stented with good outcome. To the uninitiated — this ECG may appear normal.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). RAO Caudal View Post PCI This is the RAO Caudal view after thrombectomy and stent placement. At 1605, another repeat troponin resulted at 5.271 ng/mL. RAO Caudal view: This is the RAO Caudal view. The proximal LAD is now widely patent.
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. It was stented. If you want to understand aVR, read this.]
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. A stent was placed. When the patient had chest pain, prior to nitroglycerine, what do you think the ECG showed ?
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI. QTc is the computer measurement. 100% LAD occlusion.
It was treated with and dual "kissing balloons" and drug eluting stents. Here is the post stent ECG: There is greater than 50% resolution of ST elevation (all but diagnostic of successful reperfusion) and Terminal T-wave inversion (also highly suggestive of successful reperfusion). TIMI flow is 0. Door to balloon time was 51 minutes.
He was successfully treated with one drug eluting stent. Practice putting the probe on the chest of someone with an obvious STEMI(+) OMI in order to look for regional wall motion abnormalities. Failure to consider the disease based on a patient's age will lead to missed diagnoses and worse outcomes. 1] Wereski, R., Chapman, A.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content