This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. However, one can certainly imagine that many thromboses of non-obstructive lesions completely lyse and do not leave a stenosis on same day or next day angiogram. From Gue at al.
Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. Here is the angiogram: --Culprit is 100% stenosis in the proximal RCA. Here is the angiogram: --Culprit is 100% stenosis in the proximal RCA. (It
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Most large STEMI have peak troponin I in the 20.0 Inability to recognize OMI in LBBB led to a poor outcome Learning points: 1. Next trop in AM.
The culprit lesion was a complex calcified mid LAD stenosis involving the first and second diagonal branches. Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). The case doesn't come up for quality assurance because that is only done for STEMI patients.
It was tested on a large database of known outcomes and was more than twice as senstivity as STEMI criteria and much better than cardiologists. Angiogram Culprit Lesion (s): ST elevation myocardial infarction due to 99% stenosis of the distal LAD Formal echo: Normal estimated left ventricular ejection fraction, 63%.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? His response: “subendocardial ischemia.
1-4 Surprisingly, serial angiographic studies have revealed that the plaque at the site of the culprit lesion of a future acute myocardial infarction often does not cause stenosis that, as seen on the antecedent angiogram, is sufficiently severe to limit flow. Learning Points: 1.
Barely any STE, and thus not meeting STEMI criteria. Annals of Emergency Medicine Cardiology was called to evaluate the patient immediately for emergent cath, but they stated that the ECG did not meet STEMI criteria and elected to wait for further information before proceeding with cath. He was given 6mg IV morphine for ongoing pain.
Jason asked me if I thought it is due to occlusion (without either of us knowing the outcome), and this was my answer: This is a posterolateral MI. Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. Some are STEMI-equivalents.
COPD, Idiopathic PAH, acute or chronic PE, pulmonary valve stenosis, etc) 3) Conditions affecting RV myocardial contractility, such as ARVD or RV infarction The ECGs does not really show any signs of chronic RV dilation or hypertrophy. Troponin T peaked at 2074 ng/L (very high, typical of OMI/STEMI). The LV EF was 57% at formal echo.
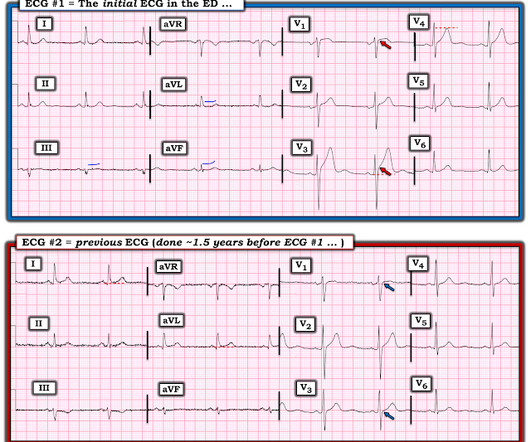
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
We have found in our study comparing inferior STEMI (manuscript in preparation) to inferior early repol several distinguishing characteristics. It showed a 99% stenosis in the RCA, and proximal to a posterolateral branch. Is this inferior ST elevation due to "early repolarization"? There is reciprocal ST depression in aVL.
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size. This difficulty results in high lateral OMI being the most commonly missed OMIs by the misguided STEMI criteria. Pride et al.
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? Appropriately, the physicians repeated the ECG 20 minutes later and it was diagnostic of anterior STEMI. Angiogram showed a critical LAD thrombotic stenosis.
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Here is an article I wrote: Updates on the ECG in ACS. see below).
Full case details and outcomes are below. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI." Case 1: Case 2: Case 1: What do you think?
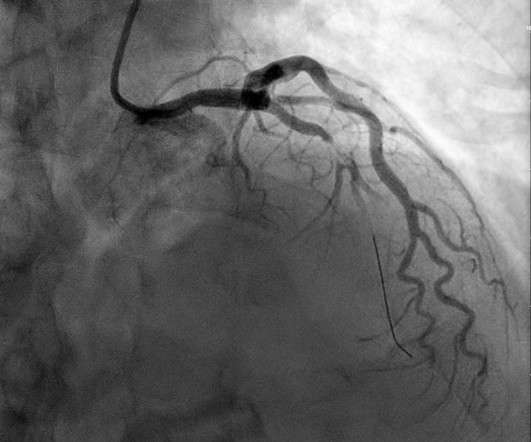
At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). The red arrow points to a 90% stenosis in the proximal segment of the LAD. Nevertheless, cases like the one presented today — illustrate the continued need for review of these points that are KEY to attaining a good outcome.
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. Type B waves are deeper and symmetric. When the patient had chest pain, prior to nitroglycerine, what do you think the ECG showed ? A stent was placed.
Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria. As has been mentioned numerous times on this site and is redemonstrated here: expert, subjective ECG interpretation is superior to STEMI criteria. Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. See these posts for Wellens' mimics: Pseudo-Wellens' Syndrome due to Left Ventricular Hypertrophy (LVH) Anterior STEMI? Am Heart J. Am J Cardiol.
ECG read as: "Shows T wave inversions in the inferior leads and less than 1mm STE in V2, without STEMI criteria." Cath was done at around 9AM: Culprit lesion mid-LAD, 99% stenosis, pre-intervention TIMI flow not listed, PCI performed with TIMI 3 flow and 0% stenosis resulting. All very very subtle. Aspirin was given.
90% stenosis of the proximal ramus intermedius, pre procedure TIMI II flow The ramus intermedius is a normal variant on coronary anatomy that arises between the LAD and LCX. Recall that air is a poor conductor of electricity and will, therefore, generate smaller amplitudes on posterior leads (hence why STEMI criteria requires only >0.5
This can only be due to STEMI. Here I annotate it: This shows 100% occluded circumflex (red arrow) and a 90% stenosis of the LAD (Yellow arrow). The LAD was thought to be not thrombotic, but a chronic tight stenosis. The LAD was thought to be not thrombotic, but a chronic tight stenosis. I said "activate the cath lab."
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. Long term outcome is unavailable. So the cath lab was activated.
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2. High sensitivity troponin I was 23 ng/L.
A reliable study would keep track of all patients with shockable arrest and analyze the ones who were not enrolled to see their outcomes. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab.
This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria. You can find the variables used to calculate the value on MD calc here: [link] Utilizing Dr. Smith’s Subtle Anterior STEMI Calculator (4-Variable), the value is greater than 18.2 which is concerning for LAD occlusion.
RBBB in acute STEMI has a very high mortality. Angiography revealed a very tight LAD stenosis with some flow (confirming the reperfusion that we see on the ECG). A stent was placed, and the patient had an excellent outcome with no wall motion abnormality. But here there is a large degree of ST elevation in V2-V6, I, and aVL.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. This ECG was recorded prehospital, and the computer read STEMI, so the medics activated the cath lab: What do you think? The ECG is consistent with high lateral STEMI. Called 911.
The is very small STE in III and aVF which do not meet STEMI criteria, hyperacute T waves, reciprocal TWI in aVL, and maximal STD in V2-V3 showing posterior OMI. The cath lab was activated despite lack of STEMI criteria, around 2 am in the morning. 33% of STEMI are reperfused by the time of angiography. Very frustrating.
Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. An EKG from a year prior was available for comparison: The ED physician noted Initial EKG here read by the computer as a STEMI, however, there is a very poor baseline and a lot of artifact. See reference and discussion below.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". A paradox in the literature: All trials of very early intervention for NSTEMI which do not exclude patients with persistent chest pain show that intervention in < 2 hours results in a better outcome. Pain was decreased to 2/10.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content