This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
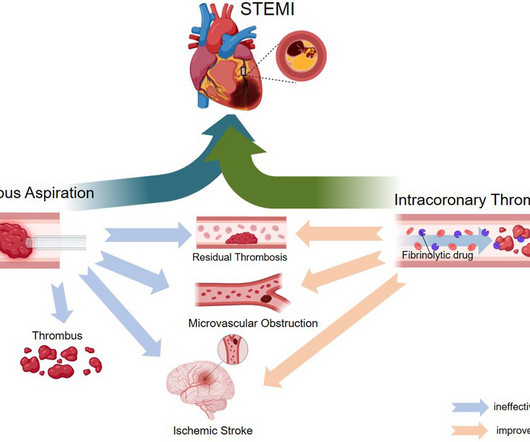
ST-elevation myocardial infarction (STEMI) is a critical cardiovascular emergency characterized by acute coronary artery occlusion and subsequent myocardial injury. However, despite successful revascularization, microvascular obstruction (MVO) remains a major challenge, contributing to adverse clinical outcomes.
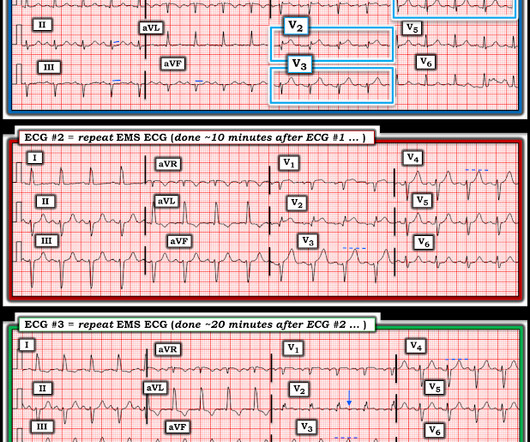
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. Long term outcome is unavailable. So the cath lab was activated.
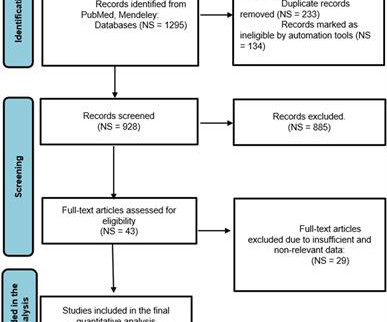
This narrative review aims to evaluate strategies for reducing door-to-balloon (D2B) time in ST-elevation myocardial infarction (STEMI) patients, focusing on pre-hospital, in-hospital, and technological innovations, as well as addressing challenges to ensure sustainability.
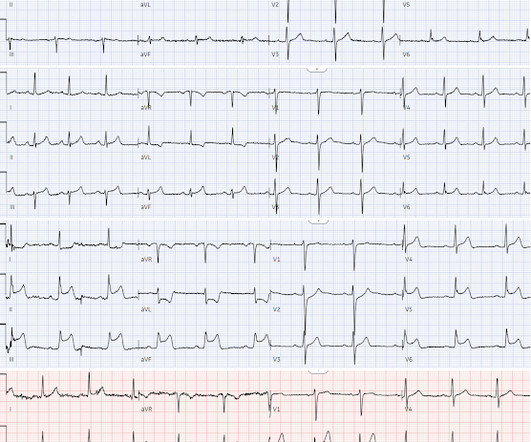
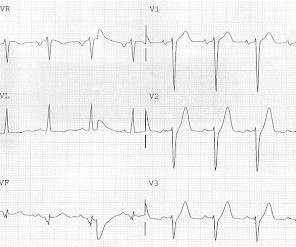
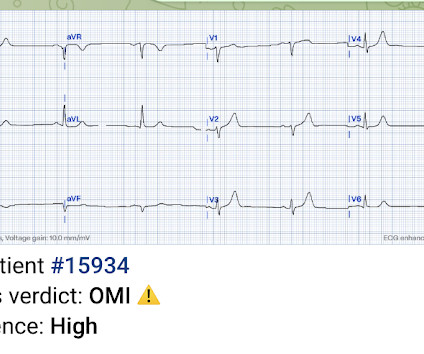
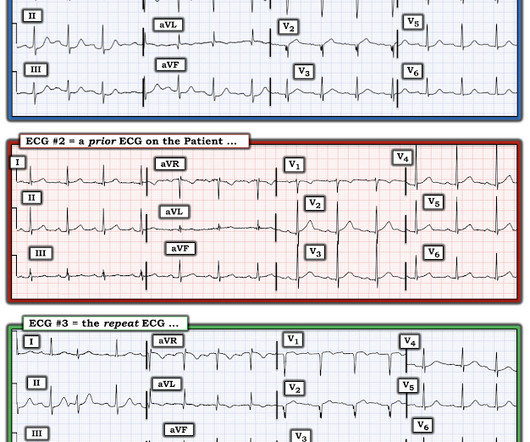
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. The patient survived with unknown long term outcome.
They concluded, "Our findings increase confidence in the normal automated GE Marquette 12 SL ECG software interpretation to predict a benign outcome. Smith comment: this is a very stupid outcome measure) What if we use that methodology for the ECG above? Despite serial ECGs being "STEMI negative", the cath lab was activated.
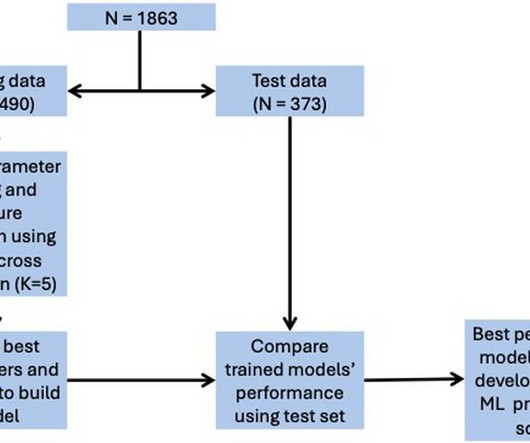
We developed a user-friendly web application for real-world use, yielding risk scores as a percentage.ConclusionsThe STEMI-ML score effectively predicts in-hospital outcomes in STEMI patients and may assist with risk stratification and individualising patient management.
What is the impact of complete revascularization versus culprit-only revascularization on outcomes in older patients with ST-segment elevation myocardial infarction (STEMI) and non–ST-segment elevation myocardial infarction (NSTEMI)?
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Opiates are associated with worse outcomes in Myocardial Infarction. Cath attending is aware.
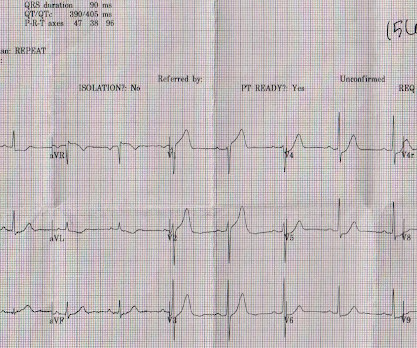
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
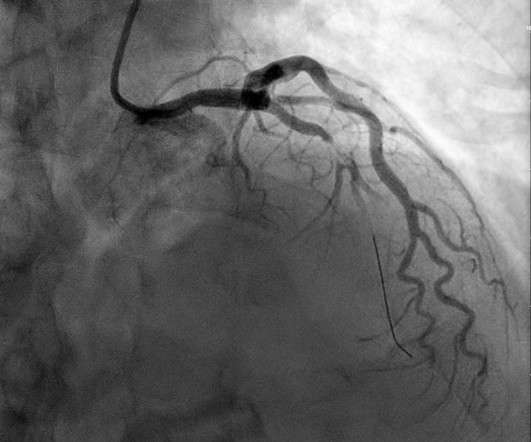
Later it was shown that index of microvascular resistance which quantified the inability of microcirculation to vasodilate and improve coronary flow after primary PCI, was associated with worst outcomes independent of epicardial coronary flow. Immediate Microvascular Physiology After Mechanical Coronary Reperfusion of STEMI.
Doing so literally enables those of us who embrace the OMI Paradigm the ability to recognize within seconds that a patient with new CP ( C hest P ain ) — and — one or more hyperacute T waves — needs prompt cath regardless of potential absence of STEMI criteria.
Cardiogenic shock (CS)is the most feared event following STEMI. We tend to perceive CS as an exclusive complication of STEMI. The incidence is half of that of STEMI, i.e., 2.5-5%. might show little elevation with considerable overlap of left main STEMI vs NSTEMI ) 2.Onset ACS pathophysiology is not that simple.
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? With serial ECGs that are ‘STEMI negative’ the physician could have waited for serial troponin levels or referred the patient as “non-STEMI”. What was the outcome and final diagnosis?
What are the outcomes of bivalirudin vs. heparin anticoagulation during percutaneous coronary intervention (PCI) in patients with ST-segment elevation myocardial infarction (STEMI)?
(MedPage Today) -- ATLANTA -- Fractional flow reserve (FFR)-guided complete revascularization in patients with ST-segment elevation myocardial infarction (STEMI) and multivessel coronary artery disease did not result in better outcomes compared.
This study shows that for a transient STEMI ("complete normalization of ST segments"), it is not unequivocally necessary to activate the cath lab emergently. This might extend to Wellens' syndrome, which is really and transient STEMI in which the ST Elevation is not recorded. See more cases of Transient STEMI here: [link]
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2. High sensitivity troponin I was 23 ng/L.
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. And as we have shown before, morphine leads to slower times to treatment and worse outcomes. 414 patients were included in the analysis.
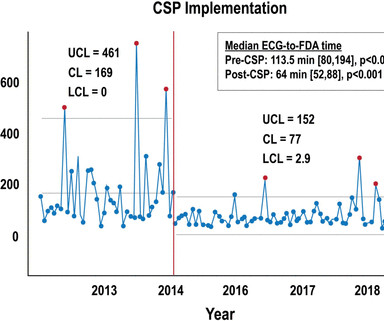
Implementing and tracking quality improvement (QI) metrics may lead to improved outcomes in patient care after STEMI in low- and middle-income countries (LMIC), according to an analysis of data from the ACC's Global Heart Attack Treatment Initiative (GHATI).
Background Hyperglycemia, characterized by elevated blood glucose levels, is frequently observed in patients with acute coronary syndrome, including ST-elevation myocardial infarction (STEMI). There are conflicting sources regarding the relationship between hyperglycemia and outcomes in STEMI patients. 3.45) and 4.47 (95% CI: 2.54–7.87),
The cath lab was activated, as it should be with transient STEMI. See this case of transient STEMI: Spontaneous Reperfusion and Re-occlusion - My Bad Thinking Contributes to a Death. Been discharged to home with potential disastrous outcome. Undergone stress test with uncertain results. Learning Points 1.
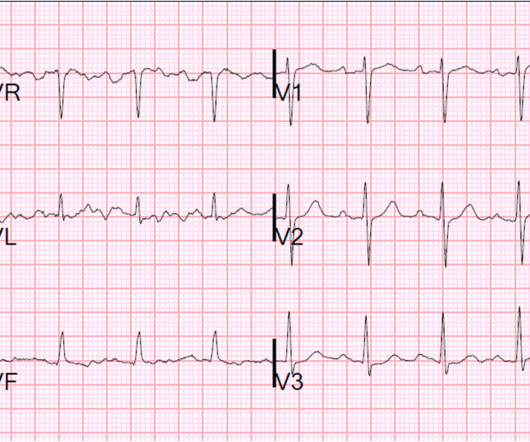
You can see how V1, V2, aVR, and V4R would have ST elevation in either a right ventricular STEMI or with a septal STEMI, and how lateral leads, and even posterior leads, would have reciprocal ST depression. of patients with anterior STEMI, ST elevation of greater than or equal to 3.0 STE in V4R is confirmatory evidence.
7, 2024 — The Society for Cardiovascular Angiography & Interventions (SCAI) recently announced the publication of the Expert Consensus Statement on the Management of Patients with STEMI Referred for Primary PCI. It synthesizes the latest evidence-based practices and provides comprehensive suggestions to enhance patient care and outcomes.
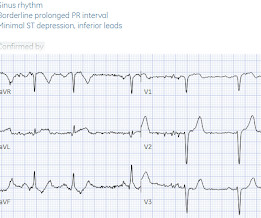
Written by Jesse McLaren Three patients presented with acute chest pain and ECGs that were labeled by the computer as completely normal, and which was confirmed by the final cardiology interpretation (which is blinded to patient outcome) also as completely normal. What do you think?
See my formula for differentiating anterior LV aneurysm (that is to say, persistent ST elevation after old MI) from acute anterior STEMI. Both support acute anterior STEMI. In fact, in our studies, the false negative cases for acute STEMI were due to prolonged occlusion (at least 6 hours). It is not chronic. 3.0 = 0.50
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Could it be acute (vs. subacute or days old)?
Posterior leads are unnecessary if anterior leads are diagnostic According to the STEMI paradigm an ECG has to have ST elevation to diagnose acute coronary occlusion, and if there’s no ST elevation on anterior leads you can look for it on posterior leads. Do you need posterior leads? If so, how will they change management?
Jason was very skeptical of STEMI. This also argues against STEMI. What was the outcome? Outcome "I later found out that this is a patient who regularly calls paramedics to c/o chest pains and he had fooled many of them. He complained of 3 days of diarrhea and abdominal pain. What do you think? Jason, I agree.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI? As cardiology documented, “possible STEMI.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Could it be acute (vs.
STEMI remains a major cause of morbidity, mortality, disability, and high health care costs in Latin America and the rest of the world. New data assessing the impact of ACC's Global Heart Attack Initiative (GHATI) on patient care outcomes at the CEDIMAT Cardiovascular Center in Santo Domingo, Dominican Republic.
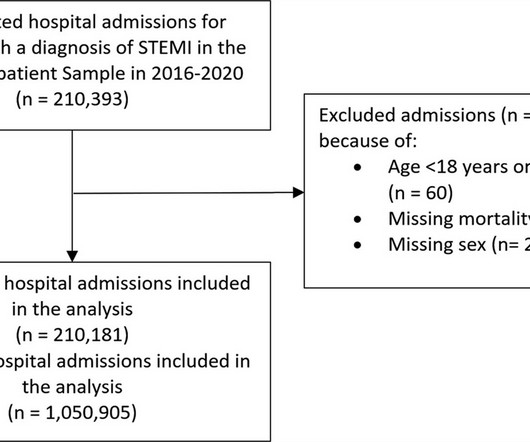
Background It is unclear how COVID-19 pandemic affected care and outcomes among patients who are diagnosed with ST-elevation myocardial infarction (STEMI) in the USA. Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2% Results There were 1 050 905 hospitalizations with STEMI, and there was an 8.2%
This systematic review of the literature aims to explore outcomes in the patients treated with conservative management vs. invasive strategy. with ST elevated myocardial infarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. Approximately 48.5%
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. We don't know how many though.
He had an immediate ED ECG: There is artifact, but the findings appear to be largely gone now The diagnosis is acute MI, but not STEMI. Outcome : Was it RCA or LCX with inferior MI? His pain was intermittent and he was vague about when it was present and when it was resolved. Here is his prehospital ECG: Diagnosis?
The most common clinical presentation of ACS was STEMI in 47.4%. The prevalence of composite clinical outcomes including mortality, non-fatal MI and recurrent SCAD was 3.3% (95% CI: 1.4–5.1), The prevalence of composite clinical outcomes including mortality, non-fatal MI and recurrent SCAD was 3.3% (95% CI: 1.4–5.1),
Introduction:Elevated LDL cholesterol is linked to microvascular injury and adverse cardiac events in STEMI patients. This study examines the impact of prior statin use on LDL levels at the time of MI, focusing on NSTEMI and STEMI patients. For STEMI, the treated group had an average LDL level of 87.8 ± 42 mg/dL versus 103 ± 41.2
BackgroundThe pharmacoinvasive (PhI) strategy is the standard-of-care for ST-elevation myocardial infarction (STEMI) patients when primary percutaneous coronary intervention (pPCI) is unfeasible. Multivariable logistic regression models were used to assess the association between lysis-PCI timing and outcomes.
1-3] But these studies were very short duration and used cardiology interpretation of ECGs or emergent angiography rather than patient outcomes. 4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6]
Background:The computational pressure-fluid dynamics applied to index of microcirculatory resistance, derived from coronary angiography (CPFD-caIMR) is a promising alternative method of IMR to evaluate the prognosis of STEMI patients. All patients with STEMI underwent CPFD-caIMR and MVO assessment.
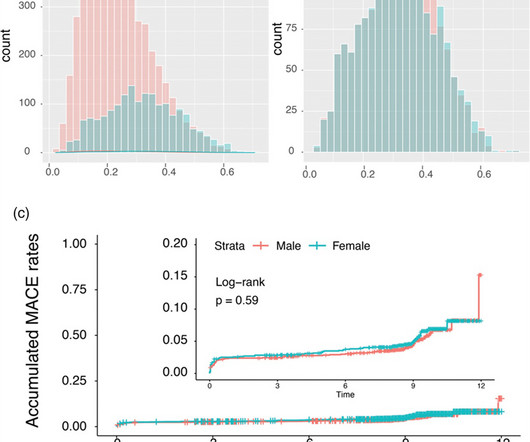
Background: Gender-specific outcomes after percutaneous coronary interventions were studied by a number of research groups with different endpoints and cohorts of different ethnic extractions. In the unmatched STEMI subgroup, all-cause mortality was significantly higher in females driven by older age (P < 0.001). vs. 3.9%; P = 0.020).
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content