This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Peak troponin, echocardiographic findings, and long term outcome are unknown. A new right bundle branch block in a sick patient with chest pain and/or shortness of breath is a worrisome finding concerning for LAD occlusion or significant pulmonary embolism. Learning Points: 1.
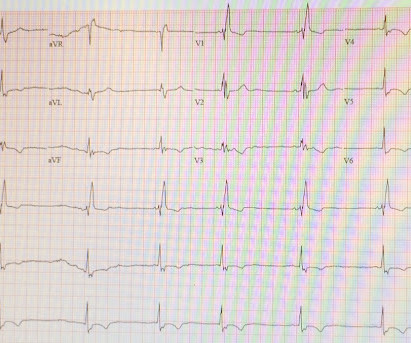
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of Chest Pain and Dyspnea Head On Motor Vehicle Collision. Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). ST depression. Myocardial Contusion?
CT pulmonary angiogram was negative for pulmonary embolism. Learning Points It takes dedicated learning and observation of outcomes and serial ECGs to learn how to distinguish subtle OMI patterns from OMI mimics like the cases above. Second troponin T resulted at 1,318 ng/L. Chest x-ray was read as normal. Heparin was started.
The VARIPULSE Platform is designed to enable pulmonary vein isolation with the versatility of a catheter loop, a simple generator user interface, and a mapping system that provides an intuitive, reproducible workflow with real-time visualization, contact indicator, and PF tagging mechanisms. In: AF Symposium.; February 2-4; Boston.
Patients with paroxysmal or persistent atrial fibrillation underwent pulmonary vein (PV) isolation under deep sedation or general anesthesia and returned for remapping at 90 days to evaluate chronic durability. Circulation: Arrhythmia and Electrophysiology, Ahead of Print. paroxysmal, and 58.5% deep sedation) were treated.
such Q-waves are associated with larger MI and worse outcomes (2. When there is MI extending all the way to the epicardium (transmural), that infarcted epicardium is often inflamed (postinfarction regional pericarditis, or PIRP). What complication is the patient with post-infarction regional pericarditis at risk for?
and these are associated with larger MI and worse outcomes (2. When there is MI extending all the way to the epicardium (transmural), that infarcted epicardium is often inflamed (postinfarction regional pericarditis, or PIRP). Although the patient has had pain for 4 days, could the artery have fully occluded only within hours?
The initial computer and final cardiology interpretation was a differential: “ST elevation, consider early repolarization, pericarditis, or injury.” But STEMI criteria ignore all this and look at ST segments in isolation. Based on STEMI criteria and unhelpful computer interpretation, the patient was rushed to the cath lab.
CT angiogram chest: no aortic dissection or pulmonary embolism. Serial chest xrays: progressive bilateral pulmonary edema. Smith Major Learning Point: The worst risk factor for a bad outcome in OMI is young age because cardiologists cannot believe that a young person can have an OMI. Pericarditis?
The exception is with postinfarction pericarditis , in which a completed transmural infarct results in inflammation of the subepicardial myocardium and STE in the distribution of the infarct, and which results in increased STE and large upright T-waves. These findings together are more commonly seen with pericarditis.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content