This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Acute pericarditis (AP) is the second most common cardiac cause of chest pain, diagnosed when at least two of the following criteria are met: characteristic pleuritic chest pain, pericardial rub on auscultation, new typical ECG changes (such as widespread ST-elevation or PR-depression) and pericardial effusion on imaging.
(MedPage Today) -- Only myocarditis/pericarditis and seizures occurred at higher rates in adolescents and children vaccinated for COVID-19 when compared with historical rates of those outcomes, according to an analysis of safety data from the FDA.
They included randomised controlled trials that enrolled adults undergoing major cardiac surgeries and reported postpericardiotomy syndrome, pericardial effusion and pericarditis as primary or secondary outcomes. to 0.81) and may prevent postoperative pericarditis (RR 0.66, 95% CI 0.45 95% CI 0.20 to 0.97) compared with control.
Background There are limited data on acute pericarditis according to different age groups. The aim of this study is to investigate the role of age-related features in clinical characteristics, management, and outcomes of acute pericarditis, with a focus on the geriatric population. and G4: 16.2%; p<0.001).
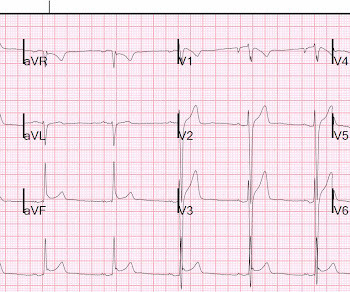
The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.” The final cardiology interpretation confirmed the computer interpretation of “ST elevation, consider early repolarization, pericarditis or injury”. A healthy 45-year-old female presented with chest pain, with normal vitals.
Clinician and EKG machine read of acute pericarditis. While it is true that inferior MI has ST depression in aVL 99% of the time (Bischof and Smith), and that inferolateral ST elevation is the most common distribution for pericarditis, the ST elevation in V3 has "terminal QRS distortion (TQRSD)," (diagnostic of LAD occlusion).
TB pericarditis is the commonest cardiac manifestation of TB and is the leading cause of constrictive pericarditis, a reversible (by surgical pericardiectomy) cause of diastolic heart failure in endemic areas. Subsequently, risk stratification strategies for constrictive outcomes have remained unsatisfactory.
06:44 - T-waves in V2 are smaller now - Overall resolution of prior findings (which qualifies as a dynamic change) The initial note by the cardiologist states that the presentation is more consistent with pericarditis. Remember, pericarditis is the thing you say and write down when youre actively trying to miss an OMI.
Recurrent pericarditis (RP) is the most troublesome complication of acute pericarditis reflecting an unresolving inflammation of the pericardial sac around the heart and associated with significant morbidity.
There is a reasonable chance of pericarditis in this case, or this could be a baseline." Other outcome information is not available. Sadly, I did not receive enough information to adjudicate whether this patient has pericarditis or not. But I would cath unless there is some clear clinical feature that points to pericarditis.
There were no incidences of adverse event fistula, diaphragmatic paralysis, MI, pericarditis, thromboembolism, PV stenosis, transient ischemic attack, or death. Circulation: Arrhythmia and Electrophysiology, Ahead of Print. BACKGROUND:Pulsed field ablation (PFA) is a promising treatment for atrial fibrillation.
such Q-waves are associated with larger MI and worse outcomes (2. When there is MI extending all the way to the epicardium (transmural), that infarcted epicardium is often inflamed (postinfarction regional pericarditis, or PIRP). What complication is the patient with post-infarction regional pericarditis at risk for?
Below is the first ECG, signed off by the over-reading cardiologist agreeing with the computer interpretation: ST elevation, consider early repolarization, pericarditis, or injury. Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. What do you think?
and these are associated with larger MI and worse outcomes (2. When there is MI extending all the way to the epicardium (transmural), that infarcted epicardium is often inflamed (postinfarction regional pericarditis, or PIRP). Although the patient has had pain for 4 days, could the artery have fully occluded only within hours?
Twelve-month outcomes data from the pilot phase of the admIRE study, which assessed the safety and efficacy of the VARIPULSE Platform among U.S. Pulsed Field Ablation Using a Variable Loop Circular Catheter with 3D Mapping Integration: Early Outcomes of the admIRE Study [abstract]. In: AF Symposium.; February 2-4; Boston.
These latter findings are typical of pericarditis, but pericarditis never has reciprocal ST depression. Usually with pericarditis and myocarditis — hyperacute T waves (HATW) are not present. S mith : there is STE in lead III and reciprocal STD in aVL. This is OMI until proven otherwise.
Post-infarction Regional Pericarditis (PIRP) PIRP happens when MI is transmural, all the way from subendocardium to subepicardium, thus leading to inflammation of the subepicardium (next to the pericardium). MYOCARDIAL RUPTURE AND POSTINFARCTION REGIONAL PERICARDITIS KEY POINTS · Myocardial rupture occurs in 1 to 1.5% Re-occlusion 2.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." St depression in lead AVL differentiates inferior st-elevation myocardial infarction from pericarditis. link] Bischof, J. Worrall, C.,
Traditionally used as an anti-inflammatory for pericarditis (inflammation of the lining of the heart), it has recently been shown to result in fewer major heart events in those with a recent heart attack. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. It is an easy win, frequently missed. N Engl J Med.
Queen of hearts interpretations: Patient 1, ECG1: Patient 2, ECG1: Patient 1 Clinical Course and Outcome: The EM physician did not see that the S wave voltage has been truncated and squared off at 10 mm, thereby greatly limiting the assessment of proportionality. He diagnosed anterior "STEMI" and activated the cath lab. But he did well.
T-wave to ST ratio is greater than 4 in lead V6, making pericarditis unlikely (also there were no symptoms of pericarditis). Long-term outcome associated with early repolarization on electrocardiography. There is ST elevation diffusely: 2 mm in V2, 3.5 mm in V3, 2.5 mm in V4, 1.5 mm in V5, and 1 mm in V6, 1.5
Peak troponin, echocardiographic findings, and long term outcome are unknown. On day 3 of hospitalization she underwent coronary angiography, revealing a 95% lesion in the mid-LAD which was stented. One can say with full confidence that is was completely occluded at the time of the presentation ECG. Learning Points: 1.
Pericarditis is rare — but myocarditis is not , so especially in this age group — more information is needed to quickly determine if this could be an acute MI, myocarditis, or none of the above. To quote Dr. Stephen Smith: "The worst risk factor for a bad outcome in acute MI is young age."
ECG of pneumopericardium and probable myocardial contusion shows typical pericarditis Male in 30's, 2 days after Motor Vehicle Collsion, complains of Chest Pain and Dyspnea Head On Motor Vehicle Collision. Atrial fibrillation is also a predictor of worse outcomes in this case (Alborzi). ST depression. Myocardial Contusion?
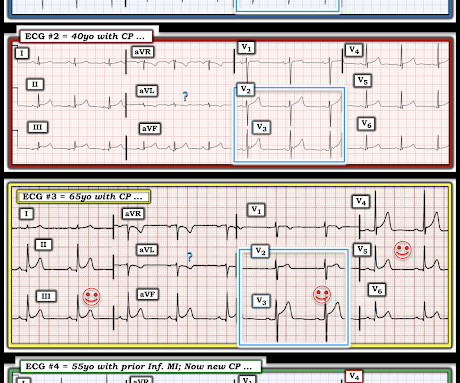
ECG#1 ECG#2 ECG#3 ECG#4 ECG#5 See outcomes of all 5 below, with the Queen of Hearts AI Bot interpretation. All of the patients presented with chest pain , and they are all in triage. Which, if any, of these patients has OMI, with myocardium at risk and need for emergent PCI? YOU TOO CAN HAVE THE PM Cardio AI BOT!!
As always, takotsubo cardiomyopathy and focal pericarditis can mimic OMI, but takotsubo almost never mimics posterior MI, and both are diagnoses of exclusion after a negative cath. Could this outcome have been prevented with emergent cath? His first troponin returned "elevated" (level not available).
Smith Major Learning Point: The worst risk factor for a bad outcome in OMI is young age because cardiologists cannot believe that a young person can have an OMI. Pericarditis? He was readmitted a few weeks later for a heart failure exacerbation, diuresed, and discharged again. This gets drilled into them.
False Positive ST elevation in aVL Even when the story is obvious, with intractable pain, the STEMI paradigm can cause preventable delays Man in his 60's with very subtle ECG and pain not controlled with medical therapy Pericarditis vs. MI #2 See other "Quiz Posts": Quiz post - which of these, if any, are OMI? Will you activate the cath lab?
To-date no larger studies have assessed sub-clinical myocardial mechanics in acute tuberculous pericarditis (ATBP) and age/sex/ethnic differences, and synergistic-prognostic association of these parameters with patients' outcomes (survival).Aim:To
The initial computer and final cardiology interpretation was a differential: “ST elevation, consider early repolarization, pericarditis, or injury.” But STEMI criteria ignore all this and look at ST segments in isolation. Based on STEMI criteria and unhelpful computer interpretation, the patient was rushed to the cath lab.
The exception is with postinfarction pericarditis , in which a completed transmural infarct results in inflammation of the subepicardial myocardium and STE in the distribution of the infarct, and which results in increased STE and large upright T-waves. These findings together are more commonly seen with pericarditis.
In addition, ischemic STD in aVL is highly sensitive for inferior OMI, and excludes pericarditis. for both pericarditis and normal variant, the vector results in more STE in II than III, and absence of STD in aVL. It means that, if there is STD in aVL, then it is almost certainly not pericarditis (but could be myocarditis).
Background Studies predating widespread COVID-19 vaccination identified patients with congenital heart disease (CHD) as a group at increased risk of severe outcomes from COVID-19. Here we evaluate the impact of vaccination on COVID-19 outcomes among patients with CHD.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content