This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
narrates and is a co-producer of a documentary focused on radiation and orthopedic injuries suffered by doctors and nurses who work in cardiac catheterization laboratories where they apply the very latest non-surgical technologies to treat the world’s leading cause of death, heart disease. Rizik , M.D., Diethrich , M.D.,
Drug-eluting stents (DES) play a crucial role in treating coronary artery disease (CAD) by preventing restenosis. These stents are coated with drug carriers that release antiproliferative drugs within the vessel. The most cited document pertained to standardized definitions for clinical endpoints in coronary stent trials.
Background:A new policy was implemented in November 2021 to reduce the length of post-anesthesia-care-unit (PACU) stay from 6 hours to 4 hours to reduce the nursing care burden and decrease the length of stay, yet how it affected patients’ events after PACU discharge needed close evaluation.
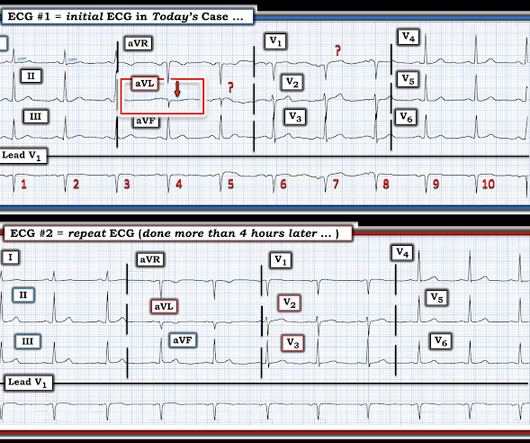
Nurse notes: the silent scream of the heart The emergency nursing notes document the patient complaining of chest pain refractory to nitro, with a rising trop: 2200: ECG shown to ED MD 0020: repeat ECG shown to ED MD, patient complain of midsternal chest pain 0520: nitro x 3.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The patient underwent successful placement of one drug eluting stent with restoration of TIMI 3 flow.
Triage is backed up, and 10 minutes into your shift one of the ED nurses brings your several ECG s that has not been overread by a physician. The patient was referred immediately for cath which revealed RCA occlusion that was stented. Imagine you just started your ED shift. It's a busy Friday afternoon.
In spite of aggressive questioning, he denied chest pain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4. An open 90% LAD was stented. He had been awakened by cough at 3 AM 2 days earlier.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic @DidlakeDW A 50 y/o Male was taking his dog for a leisurely stroll through the park when he suddenly experienced new onset chest discomfort. One stent was deployed with restorative TIMI-0 flow. However, when the Troponin I returned 8.4
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith @SmithECGblog I was conducting QA/QI on two very recent cases and was struck by the uniqueness of both. He was rushed to the Cath Lab where an LAD culprit lesion was stented. Here is the LAD after stent placement.
She contacted her neighbor, a nurse, for help. Here is the angiogram after stent placement. She eventually fell back asleep, and woke up feeling normal the next day (the day of presentation). After dinner the day of presentation, she had left neck and elbow pain which she described as dull, achy, and worse with exertion.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (Ret) @DidlakeDW Expert contribution by Dr Robert Herman @RobertHermanMD @PowerfulMedical (Chief Medical Officer) An adult male called 911 for new-onset epigastric burning. Fire/EMS crews found him clammy and uncomfortable. No appreciable skin pallor.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Expert commentary provided by Dr. Ken Grauer CASE 1 An 82 y/o Male called 911 for sudden onset dizziness while at rest. A 99% LAD occlusion was stented. Upon arrival he was found alert and oriented, and without gross distress. Attached is the first ECG.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review and commentary by Dr. Steve Smith [link] @SmithECGblog It is early-summer, approximately 1330 hours, no cloud cover overhead, and 86 degrees with high humidity. A mid-LAD culprit lesion was identified and stented.
Finally she saw a cardiologist who confirmed that she did indeed have heart failure and needed to start some medications as soon as possible and he would arrange for a heart failure nurse to see her. How can you possibly build rapport and trust if you never see the same doctors/ nurses more than once?
This was stented. It would be difficult to get a nurse to give it faster! During the resuscitation, I ordered 10 mEq KCl push, but the patient received 40 mEq of KCl, push (far more than recommended) The resident had ordered 40 mEq and that is what the nurses heard. After pacing, there was no recurrence of Torsades.
The nurse alerted the MD because the patient was still symptomatic, diaphoretic and “looking unwell”. After the episode of VT and the troponin results the patient was taken to the cath lab: complete occlusion of the RCA with TIMI 0 flow, which was stented. What do you think? He also had 70% lesion of his LAD.
A third EKG was obtained at 0144 because nursing staff noticed changes in ST elevation on the patients monitor: There is now a tremendous 6-7mm of ST Elevation in lead III! It was treated with a drug eluting stent. The Marquette 12 SL algorithm again only noted LBBB. The Queen of hearts also recognizes this ECG as OMI.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. Pretty impressive for someone who has not yet attended med school, or even been a nurse or paramedic yet. He had an EKG recorded right away.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content